

Text Description
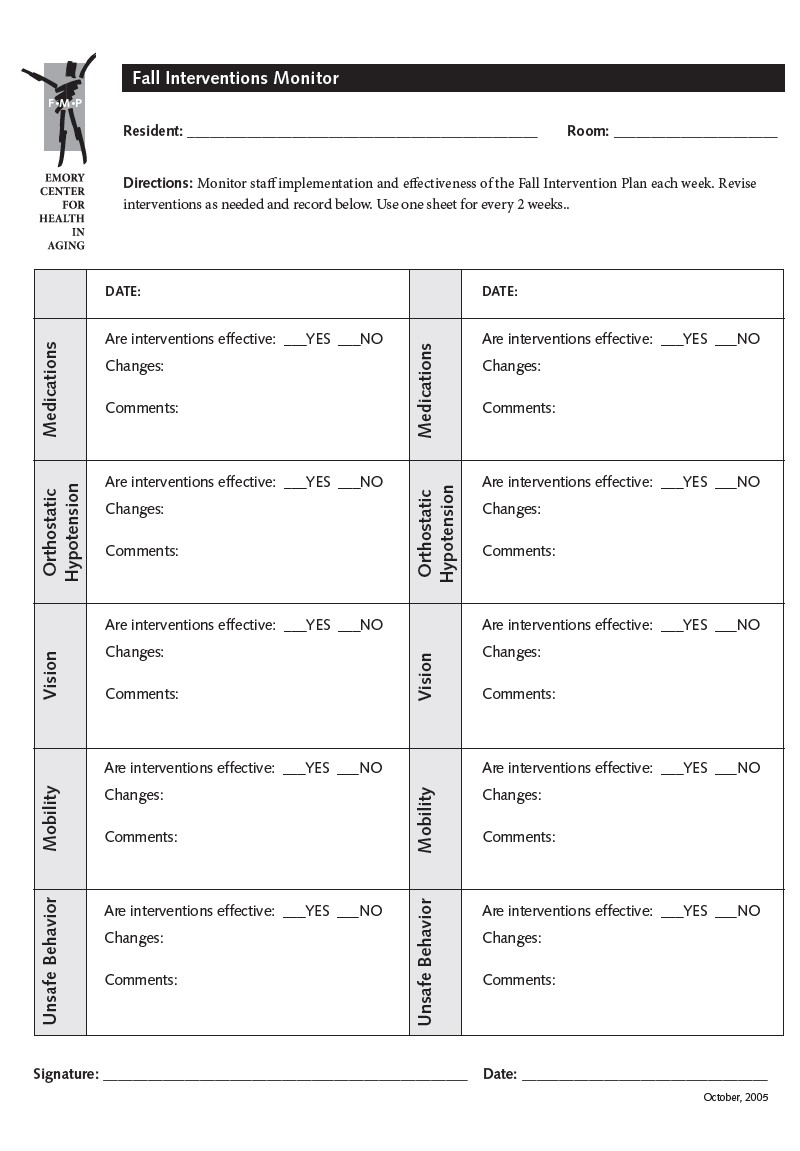
Resident: _____________________________________________ Room: ____________________
Directions: Monitor staff implementation and effectiveness of the Fall Intervention Plan each week. Revise interventions as needed and record below. Use one sheet for every 2 weeks.
| Date: | Date: | ||
|---|---|---|---|
| Medications |
Are interventions effective: ___ Yes ___ No Changes: Comments: |
Medications |
Are interventions effective: ___ Yes ___ No Changes: Comments: |
| Orthostatic Hypotension |
Are interventions effective: ___ Yes ___ No Changes: Comments: |
Orthostatic Hypotension |
Are interventions effective: ___ Yes ___ No Changes: Comments: |
| Vision |
Are interventions effective: ___ Comments: |
Vision |
Are interventions effective: ___ Yes ___ No Changes: Comments: |
| Mobility |
Are interventions effective: ___ Yes ___ No Changes: Comments: |
Mobility |
Are interventions effective: ___ Yes ___ No Changes: Comments: |
| Unsafe Behavior |
Are interventions effective: ___ Yes ___ No Changes: Comments: |
Unsafe Behavior |
Are interventions effective: ___ Yes ___ No Changes: Comments: |
Signature: _________________________________________ Date: ___________________________