

Amplify Your Impact on Child Health Care Quality
Learning from the CHIPRA Quality Demonstration Grant Program
On February 11, 2016, AHRQ and CMS presented a free Webinar, "Amplify Your Impact on Child Health Quality: Learning from the CHIPRA Quality Demonstration Grant Program." The presentations featured highlights and a discussion of promising practices and key lessons learned from the 5-year demonstration grant program to improve health care quality for children in Medicaid and CHIP. The slide deck from that Webinar is available as a separate file (PDF File, 1.1 MB)
Slide 1
Amplify Your Impact on Child Health Care Quality:
Learning from the CHIPRA Quality Demonstration Grant Program
Webinar
February 11, 2016
This title slide also includes the logos for the Agency for Healthcare Research and Quality, the Centers for Medicare & Medicaid Services, Mathematica Policy Research, the National Evaluation of the CHIPRA Quality Demonstration Grant Program, and AcademyHealth.
Slide 2
Agenda
- Welcome and introductions: Renee Fox, CMS, and Linda Bergofsky, AHRQ.
- Overview of the demonstration, the national evaluation, and the customized technical assistance opportunity: Linda Bergofsky, AHRQ.
- Lessons from the demonstration
- Transforming primary care practices and using quality measures: Joe Zickafoose, Mathematica.
- Q&A.
- Improving systems for youth with complex behavioral health care needs, and using partnerships and coalitions: Grace Anglin, Mathematica.
- Q&A.
- Perspectives from a non-demonstration State: Henry Ireys, Mathematica, and Jeff Schiff, Minnesota Health Care Programs.
- Q&A and recap.
Slide 3
Children's Health Insurance Program Reauthorization Act (CHIPRA) of 2009
- CHIPRA 2009 established the CHIPRA Quality Demonstration Grant Program and its evaluation
- $100 million grant program: one of the largest federal efforts to focus on health care for children.
- Purpose: to examine promising ideas for improving the quality of children's health care provided under Medicaid and CHIP.
- 10 five-year grants awarded by CMS
- 18 states with demonstration dollars (6 multi-state partnerships).
- February 2010–February 2015.
Slide 4
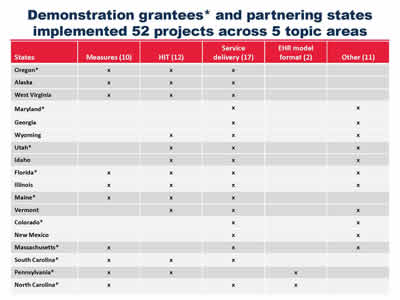
Demonstration grantees* and partnering states implemented 52 projects across 5 topic areas
| States | Measures (10) | HIT (12) | Service delivery (17) | EHR model format (2) | Other (11) |
|---|---|---|---|---|---|
| Oregon* | X | X | X | ||
| Alaska | X | X | X | ||
| West Virginia | X | X | X | ||
| Maryland* | X | X | |||
| Georgia | X | X | |||
| Wyoming | X | X | X | ||
| Utah* | X | X | X | ||
| Idaho | X | X | X | ||
| Florida* | X | X | X | X | |
| Illinois | X | X | X | X | |
| Maine* | X | X | X | ||
| Vermont | X | X | X | ||
| Colorado* | X | X | |||
| New Mexico | X | X | |||
| Massachusetts* | X | X | X | ||
| South Carolina* | X | X | X | ||
| Pennsylvania* | X | X | X | ||
| North Carolina* | X | X | X |
Slide 5
National Evaluation
- Purpose: To provide insight into best practices and replicable strategies for improving the quality of children's health care.
- National Evaluation Team
- Mathematica, Urban Institute, AcademyHealth.
- CMS funding, AHRQ oversight.
- August 2010 – September 2015.
- Continuation of the National Evaluation
- Focused on updating and disseminating lessons.
- Mathematica, AcademyHealth.
- October 2015 – June 2017.
Slide 6
Evaluation Results
- AHRQ-hosted website: http://www.ahrq.gov/policymakers/chipra/demoeval/index.html
- Final and summary reports.
- Reports and resources from the States.
- 18 State Spotlights, 13 Evaluation Highlights, 2 Implementation Guides.
- Journal manuscripts.
- Special innovation features.
Slide 7
Broad Lessons from the Demonstration
- CHIPRA quality demonstration grants played a vital role
- Helped to keep children on State policy agendas.
- Demonstrated QI strategies to key policymakers.
- Brought "intellectual capital" to States
- Substantial experience.
- Application of innovative ideas.
- New or strengthened partnerships.
- "Dividends" continue in 12 States
- New scope-of-work provisions in State-university contracts.
- New units in State Medicaid agencies.
- Continued funding for statewide partnerships.
Slide 8
Customized Technical Assistance to Improve the Quality of Children's Health Care:
Learn from the Demonstration States' Experience.
Slide 9
Technical Assistance and Knowledge Transfer
- Information about technical assistance/knowledge transfer opportunity: http://www.ahrq.gov/policymakers/chipra/demoeval/whatsnew.html#ta.
- Goal: Apply lessons from the demonstration and increase successful outcomes for children.
- Eligibility: Non-demonstration states and partner organizations.
- Support: Team of experts, State peer-to-peer learning, no direct funding.
- Duration: April 2016 – March 2017.
Slide 10
Lessons from the Demonstration
- Transforming primary care for children.
- Using child health care quality measures.
- Improving systems for youth with complex behavioral health care needs.
- Using partnerships and coalitions.
Slide 11
Primary Care Transformation in CHIPRA States
- 12 States worked with primary care practices.
- 2 States worked with 22 school based-health centers.
- Diverse strategies
- Learning collaboratives.
- Technical assistance & practice facilitation.
- Care coordination.
- Family engagement.
Slide 12
Practice Transformation Strategies (1)
Learning collaboratives
- Incentives for participation.
- Didactics and interactive learning.
- Peer networking.
- Alignment with other strategies.
Technical assistance & practice facilitation
- Tailor efforts to practice.
- Support QI measurement and feedback.
- External vs. internal facilitation.
This slide includes boxes for lessons about learning collaboratives and technical assistance and practice facilitation.
Slide 13
Practice Transformation Strategies (2)
Care coordination
- Promote concepts.
- Support for functions and dedicated staff.
- External staff.
Family engagement
- Parent advisors.
- Peer support.
- Surveys and focus groups.
This slide includes boxes for lessons about care coordination and family engagement.
Slide 14
Knowledge Transfer Examples
- Primary care transformation
- Designing or adapting state-sponsored primary care learning collaboratives.
- Developing an approach to practice facilitation.
- Quality measures.
- Youth with complex behavioral health care needs.
- Partnerships and collaborations.
The figure displays examples of knowledge transfer opportunities, focused on primary care transformation. Examples include (1) designing or adapting State-sponsored primary care learning collaboratives and (2) developing an approach to providing practice facilitation.
Slide 15
Lessons from the Demonstration
- Transforming primary care for children.
- Using child health care quality measures.
- Improving systems for youth with complex behavioral health care needs.
- Using partnerships and coalitions.
Slide 16
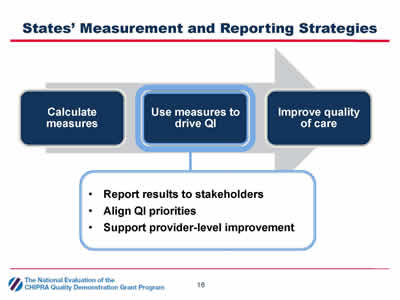
States' Measurement and Reporting Strategies
- Calculate measures.
- Use measures to drive QI:
- Report results to stakeholders.
- Align QI priorities.
- Support provider-level improvement.
- Improve quality of care.
This slide depicts a flowchart showing the progression in measurement and reporting strategies used by demonstration States. It reads from left to right: from calculate quality measure, to use measures to drive quality improvement, to improve quality of care. A drop-down box emphasizes how States used measures to drive quality improvement by reporting results to stakeholders, aligning quality improvement priorities, and supporting provider-level improvement.
Slide 17
Reporting Results to Stakeholders
- CHIPRA State strategies
- Produce reports from:
- Administrative data (Medicaid claims, immunization registries).
- Practice data (manual chart reviews, EHRs).
- Develop reports for different audiences: policymakers, health plans, providers, the public.
- Produce reports from:
Slide 18
Aligning QI Priorities
- CHIPRA State strategies
- Convened multi-stakeholder QI workgroups.
- Encouraged consistent quality reporting standards across programs.
- Required managed care organizations to meet quality benchmarks.
Slide 19
Supporting Provider-Level Improvement
- CHIPRA State strategies
- Technical support
- Learning collaboratives.
- Individualized technical assistance.
- Financial support
- Paid providers for reporting measures and demonstrating improvement.
- Changed reimbursement practices to support improvements.
- Technical support
Slide 20
Knowledge Transfer Examples
- Primary care transformation
- Designing or adapting state-sponsored primary care learning collaboratives.
- Developing an approach to practice facilitation.
- Quality measures
- Adjusting measure specifications for practice-level reporting.
- Engaging target audiences to design quality reports.
- Youth with complex behavioral health care needs.
- Partnerships and collaborations.
The slide presents examples of ways to promote knowledge transfer in the areas of primary care transformation through learning and practice facilitation and the use of quality measures by adjusting measure specifications for practice-level reporting and engaging target audiences in the design of quality reports.
Slide 21
Q&A
Slide 22

Lessons from the Demonstration
- Transforming primary care for children.
- Using child health care quality measures.
- Improving systems for youth with complex behavioral health care needs.
- Using partnerships and coalitions.
Slide 23
What Are Care Management Entities?
- Multiple agencies serve youth with complex behavioral health needs
- Poorly coordinated services → Lower quality and higher costs.
- CMEs help families better manage cross-agency services.
- CMEs are structured differently but follow common wraparound principles
- Connect families with a care coordinator.
- Develop family-driven care plans.
- Develop diverse care teams of providers and natural supports.
Slide 24
CHIPRA States' CME Work
- Maryland and Georgia refined their existing CMEs.
- Wyoming designed and piloted its first CME.
This slide includes a picture of the cover of an implementation guide titled, "Designing Care Management Entities for Youth with Complex Behavioral Health Needs," developed by the CHIPRA Quality Demonstration national evaluation team.
Slide 25
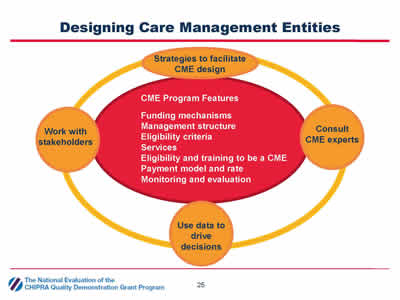
Designing Care Management Entities
The figure illustrates the program features States should consider when designing a Care Management Entity (CME) and strategies that may facilitate CME design, including funding mechanism, management structure, eligibility criteria, services, eligibility and training to be a CME, payment model and rate, and monitoring and evaluation. The strategies to facilitate CME design include working with stakeholders, consulting CME experts, and using data to drive decisions.
Slide 26
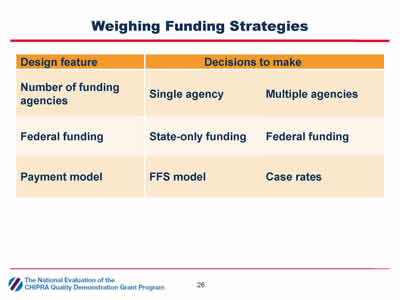
Weighing Funding Strategies
| Design feature | Decisions to make |
|---|---|
| Number of funding agencies | Single agency Multiple agencies |
| Federal funding | State-only funding Federal funding |
| Payment model | FFS model Case rates |
Slide 27

Using Data to Drive Decisions
- Administrative data analysis.
- Provider surveys.
- Interview agencies, advocacy groups, associations.
- Family and youth focus groups
- Understand current service system.
- Inform CME design decisions.
- Monitor and refine CMEs.
The figure illustrates the use of data by Care Management Entities (CMEs) to drive decisions through administrative data analysis, provider surveys, interviewing stakeholder groups, and involving family and youth focus groups. These data can help users understand the current service system, inform CME design decisions, and support CME monitoring and refinement.
Slide 28
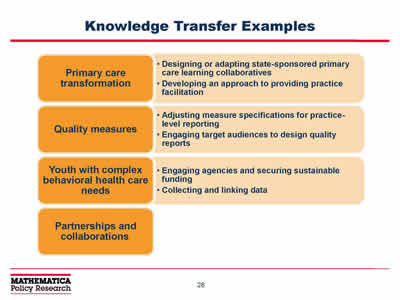
Knowledge Transfer Examples
- Primary care transformation
- Designing or adapting state-sponsored primary care learning collaboratives.
- Developing an approach to providing practice facilitation.
- Quality measures
- Adjusting measure specifications for practice-level reporting.
- Engaging target audiences to design quality reports.
- Youth with complex behavioral health care needs
- Engaging agencies and securing sustainable funding.
- Collecting and linking data.
- Partnerships and collaborations.
The figure presents examples of ways to facilitate knowledge transfer in the areas of primary care transformation, use of quality measures, and services for youth with complex behavioral health care needs. Highlighted examples include designing State-sponsored primary care learning collaboratives, providing practice facilitation, adjusting measure specifications, engaging target audiences, securing sustainable funding, and collecting and linking data.
Slide 29

Lessons from the Demonstration
- Transforming primary care for children.
- Using child health care quality measures.
- Improving systems for youth with complex behavioral health care needs.
- Using partnerships and coalitions.
Slide 30
Stakeholder Engagement in CHIPRA States
- Time-limited groups advised demonstration staff.
- Ongoing groups prioritized efforts to improve the quality of children's health care.
This slide includes a picture of the cover of an implementation guide, "Engaging Stakeholders to Improve the Quality of Children's Health Care," developed by the CHIPRA Quality Demonstration national evaluation team.
Slide 31
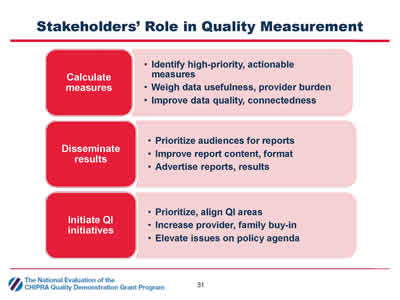
Stakeholders' Role in Quality Measurement
- Calculate measures
- Identify high-priority, actionable measures.
- Weigh data usefulness, provider burden.
- Improve data quality, connectedness.
- Disseminate results
- Prioritize audiences for reports.
- Improve report content, format.
- Advertise reports, results.
- Initiate QI initiatives
- Prioritize, align QI areas.
- Increase provider, family buy-in.
- Elevate issues on policy agenda.
The figure depicts the role of stakeholders in three areas: calculate measures, disseminate results, and initiate quality improvement initiatives. The actions for calculate measures are identify high-priority, actionable measures, weigh data usefulness and provider burden, and improve data quality and connectedness. The actions for disseminate results are prioritize audiences for reports, improve report content and format, and advertise reports and results. The actions for initiation of quality improvement activities are prioritize and align areas, increase provider and family buy-in, and elevate issues on the policy agenda.
Slide 32
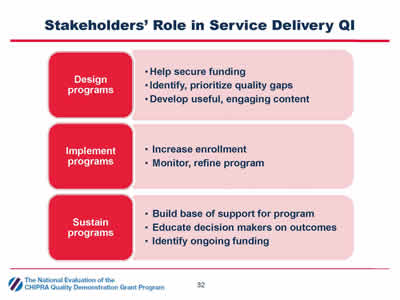
Stakeholders' Role in Service Delivery QI
- Design programs
- Help secure funding.
- Identify, prioritize quality gaps.
- Develop useful, engaging content.
- Implement programs
- Increase enrollment.
- Monitor, refine program.
- Sustain programs
- Build base of support for program.
- Educate decision makers on outcomes.
- Identify ongoing funding.
The figure illustrates the role of stakeholders in improving the quality of service delivery in three areas: program design, implementation, and sustainment. The actions for program design are secure funding, identify and prioritize quality gaps, and develop useful and engaging program content. The actions for program implementation are increase enrollment and monitor and refine the program. The actions for program sustainment are build a base of support for the program, educate decisionmakers on outcomes, and identify ongoing funding.
Slide 33
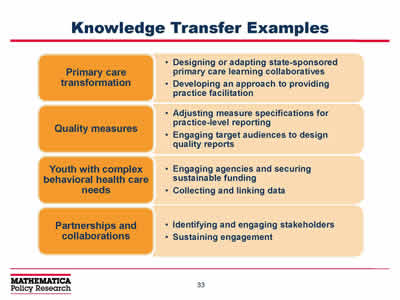
Knowledge Transfer Examples
- Primary care transformation
- Designing or adapting state-sponsored primary care learning collaboratives.
- Developing an approach to providing practice facilitation.
- Quality measures
- Adjusting measure specifications for practice-level reporting.
- Engaging target audiences to design quality reports.
- Youth with complex behavioral health care needs
- Engaging agencies and securing sustainable funding.
- Collecting and linking data.
- Partnerships and collaborations
- Identifying and engaging stakeholders.
- Sustaining engagement.
The figure provides examples of knowledge transfer opportunities for States interested in forming partnerships and collaborations, including identifying and engaging stakeholders and sustaining engagement.
Slide 34
Q&A
Slide 35
Building on Lessons from the Demonstration
Perspectives from a Non-Demonstration State
Jeff Schiff, Medical Director, Minnesota Health Care Programs, Minnesota Department of Human Services.
Henry Ireys, Project Director, National Evaluation of the CHIPRA Quality Demonstration Grant Program.
Slide 36
Questions from Dr. Schiff
- How did demonstration states work on quality with stakeholders?
- Did stakeholders include MCOs, providers, families or others?
- How did these states support quality improvement measurement and feedback to these stakeholders? What specifically did they do and how was it received?
- How did states close the feedback loop?
- How did states accomplish the task of developing and aligning QI priorities?
Slide 37
For More Information
CHIPRA Knowledge Transfer Opportunity http://www.ahrq.gov/policymakers/chipra/demoeval/whatsnew.html#ta.
CHIPRA Quality Demonstration Grant Program and National Evaluation http://www.ahrq.gov/policymakers/chipra/demoeval/index.html.
Joe Zickafoose, Project Director, Continuation of the National Evaluation, jzickafoose@mathematica-mpr.com.
Linda Bergofsky, Program Officer, Continuation of the National Evaluation, Linda.Bergofsky@ahrq.hhs.gov.