

Learn About CUSP, Facilitator Notes
CUSP Toolkit
- Slide 1. Cover Slide
- Slide 2. Learning Objectives
- Slide 3. CUSP Supports Kotter's Eight Steps of Change2
- Slide 4. CUSP Supports Kotter's Eight Steps of Change2
- Slide 5. CUSP Aligns With and Supports Other Quality and Safety Tools1
- Slide 6. CUSP is Compatible with TeamSTEPPS3
- Slide 7. CUSP is Compatible with TeamSTEPPS3
- Slide 8. Is Your Hospital Safe?
- Slide 9. Video
- Slide 10. The CUSP Model
- Slide 11. A Collaborative Effort4
- Slide 12. Toolkit Modules
- Slide 13. Toolkit Users
- Slide 14. Toolkit Users
- Slide 15. Implementation
- Slide 16. Challenges
- Slide 17. Assemble the Team
- Slide 18. Barriers to Team Performance3
- Slide 19. Engage the Senior Executive
- Slide 20. The Challenges of Partnering with a Senior Executive
- Slide 21. Understand the Science of Safety
- Slide 22. System-Level Factors Impact Safety5
- Slide 23. Identify Defects Through Sensemaking
- Slide 24. Examples of Defects or Errors That Affect Patient Safety
- Slide 25. Implement Teamwork and Communication
- Slide 26. Elements That Affect Communication and Information Exchange
- Slide 27. Apply CUSP
- Slide 28. The CUSP Model Generates Measurable Results7
- Slide 29. CUSP Results
- Slide 30. Summary
- Slide 31. References
- Slide 32. References
Slide 1. Cover Slide

Say:
The "Learn About CUSP" module of the Comprehensive Unit-based Safety Program (or CUSP) Toolkit introduces CUSP and provides an overview of resources to use when applying the CUSP model.
[D] Select for Text Description.
Slide 2. Learning Objectives
 framework and the goals of the CUSP Toolkit. 3. Demonstrate how to apply the CUSP Toolkit in a clinical environment. 4. Review the impact of errors and patient harm and the underlying causes of errors.")
Say:
This module offers an outline and brief history of the CUSP model, summarizes the CUSP Toolkit modules, and explains how to use them. In this module, we will:
- Show how CUSP supports other quality and safety tools.
- Describe the CUSP framework and the goals to achieve from using the CUSP Toolkit.
- Demonstrate how to apply the CUSP Toolkit in a clinical environment.
- Review the effects of errors and patient harm and the underlying causes of errors.
[D] Select for Text Description.
Slide 3. CUSP Supports Kotter's Eight Steps of Change2

Say:
The CUSP model supports all eight steps of the popular change model by John Kotter. The first four are:
- Step 1: Create a sense of urgency.
- Step 2: Create a guiding coalition.
- Step 3: Develop a shared vision.
- Step 4: Communicate that vision.
How do you accomplish each of these?
Aligning Kotter's change model with CUSP, the "Understand the Science of Safety" module helps you build the sense of urgency essential to inspire change among your teams. The "Assemble the Team" and "Engage the Senior Executive" modules give you templates and resources for establishing a guiding coalition to support change. "Identify Defects Through Sensemaking" helps you develop a shared vision among teams. You can communicate the concept using the tools in the "Understand the Science of Safety" and "Identify Defects Through Sensemaking" modules.
[D] Select for Text Description.
Slide 4. CUSP Supports Kotter's Eight Steps of Change2
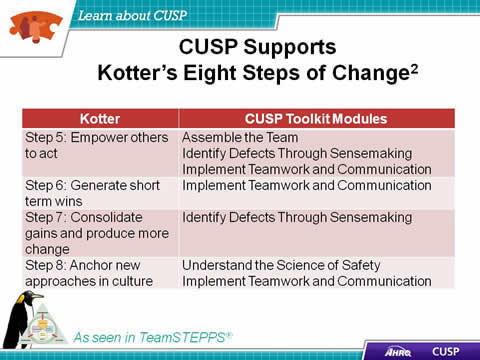
Say:
Steps five through eight of the Kotter model are:
- Step 5: Empower others to act.
- Step 6: Generate short-term wins.
- Step 7: Consolidate gains and produce more change.
- Step 8: Anchor new approaches in culture.
The CUSP Toolkit continues to coincide with Kotter's steps. How can you empower others to take action? Use the tools in the CUSP Toolkit "Assemble the Team," "Identify Defects Through Sensemaking," "Implement Teamwork and Communication," and "Understand the Science of Safety" modules.
[D] Select for Text Description.
Slide 5. CUSP Aligns With and Supports Other Quality and Safety Tools1

Say:
CUSP aligns with and supports a wide range of safety tools and approaches. When teams experience fatigue with the barrage of improvement projects, team leaders should remember to unify and streamline those initiatives by using the language of a change management framework, such as the Kotter model. Through the lens of the Kotter model, CUSP aligns with culture change and quality improvement models in the field such as:
- TeamSTEPPS®.
- Six Sigma.
- Institute for Healthcare Improvement Model for Improvement.
- Plan-Do-Study-Act, or PSDA Cycles.
- Root Cause Analysis.
- Just Culture, which is described in more detail later in this presentation..
[D] Select for Text Description.
Slide 6. CUSP is Compatible with TeamSTEPPS3

Say:
The CUSP Toolkit is compatible with TeamSTEPPS, and many of the templates and communication models in the toolkit are TeamSTEPPS tools. There are eight steps in the TeamSTEPPS model, the first four of which are:
- Step 1: Create a change team.
- Step 2: Define the problem.
- Step 3: Define the aims.
- Step 4: Design an intervention.
[D] Select for Text Description.
Slide 7. CUSP is Compatible with TeamSTEPPS3

Say:
CUSP modules also help you carry out steps five through eight of TeamSTEPPS:
- Step 5: Develop a plan for testing the effectiveness.
- Step 6: Develop an implementation plan.
- Step 7: Develop a plan for sustained improvement.
- Step 8: Develop a communication plan.
[D] Select for Text Description.
Slide 8. Is Your Hospital Safe?

Say:
There are a few questions that put the issue of patient safety in very real terms.
- Think about the unit where you work. Would you want a loved one to be a patient there? Would you want to be a patient there? Does your hospital do everything it can to protect patients?
- Do you feel comfortable talking about patient safety in your unit? Why or why not?
- When a safety issue occurs in your hospital, how does your unit address the issue?
- Is there a formal process to track safety-related improvements? Do you believe this process is effective toward improving safety within your unit?
Do:
Debrief with the group and encourage people to share their reflections. After some sharing by three or four members of the group, ask the group whether any of what was shared was surprising.
[D] Select for Text Description.
Slide 9. Video

Do:
Play the video.
[D] Select for Text Description.
Slide 10. The CUSP Model

Say:
The CUSP model was originally developed with funding from the Agency for Healthcare Research and Quality, or AHRQ, a national innovator in patient safety. CUSP dovetails with and supports a range of quality and safety improvement models.
Support from the top is crucial to the success of culture improvement efforts, but real, lasting change happens one unit at a time. Improving culture within the health care setting requires the culture model to be based on the understanding that all culture is local and that work to reform culture must be owned at the unit level. The CUSP framework accomplishes this through stressing the fact that patient harm is not an acceptable cost of doing business. Additionally, CUSP is unique in that it can be applied by anyone, anywhere, in any unit, at any time.
[D] Select for Text Description.
Slide 11. A Collaborative Effort4

Say:
The CUSP model imparts support for collaboration among providers. The earliest developments and applications of CUSP were collaborative efforts.
Teams at the Johns Hopkins Quality and Safety Research Group originally developed the CUSP model with funding from AHRQ. Dr. Peter Pronovost and leaders at Johns Hopkins were moved by the tragic death of 18-month-old Josie King from dehydration and misused narcotics at their facility, inspiring them to design and spread practices that would reduce or even eliminate the likelihood that patients would suffer harm in the course of hospital care.
Patient safety pioneers recognized early that communication and culture were key to creating safer, error-free systems. These pioneers borrowed from other high-reliability fields, like nuclear power and commercial aviation, where the use of checklists and guided communication tools were effective in reducing lapses in team functioning, errors, and the likelihood of harm.
An infection reduction project of the Michigan Health and Hospital Association Keystone Center for Patient Safety proved that CUSP was successful in improving the safety culture. In 2003, the Michigan Keystone Center launched an AHRQ-funded project to reduce central line-associated bloodstream infections in select Michigan intensive care units. The project was extremely successful, and the participating Michigan ICUs continue to sustain central line-associated bloodstream infections, or CLABSI, rates of zero percent, even today.
In 2008, AHRQ funded national projects to apply the CUSP model to reduce infections nationwide.
The toolkit is not meant to replace other safety improvement models, but to support, combine, and work in tandem with them. While these models vary in their areas of emphasis, they all align when they are viewed through the lens of an organizational change framework such as the Kotter model.
In 2009, more than 350 hospitals in 22 States reduced CLABSI rates by an average of 35 percent. All these units implemented CUSP, and many of them continue to see these rates at or near zero over extended time.
[D] Select for Text Description.
Slide 12. Toolkit Modules
Learn About CUSP. Assemble the Team. Engage the Senior Executive. Understand the Science of Safety. Identify Defects through Sensemaking. Implement Teamwork and Communication. Apply CUSP.
Say:
The CUSP Toolkit's modules are the following:
- Learn About CUSP.
- Assemble the Team.
- Engage the Senior Executive.
- Understand the Science of Safety.
- Identify Defects through Sensemaking.
- Implement Teamwork and Communication.
- Apply CUSP.
Users familiar with the original CUSP model will note this toolkit condenses two steps of the original model—"identify defects" and "learn from defects"—into the "Identify Defects Through Sensemaking" module.
We encourage new users to complete the modules in the following order for their first review:
- Understand the Science of Safety.
- Assemble the Team.
- Engage the Senior Executive.
- Identify Defects Through Sensemaking.
- Implement Teamwork and Communication.
After your initial review, there is no specific sequence in which the materials in this toolkit should be used.
For example: A year from now, a team might find their senior executive champion's interest is waning. The team can use the resources in the "Engage the Senior Executive" module to refresh their memories about processes and approaches, then apply them to regain the executive champion's commitment to the ongoing process of safety improvement.
Facilities that have previously applied CUSP, or are planning implementation on a new unit, may already understand the importance of CUSP and may have the full support of their organization's leadership. As a result, the module on assembling teams may initially be the most useful to them. In other situations, to educate those who are unfamiliar with CUSP and why it matters, the "Understand the Science of Safety" module may be more constructive.
Because different users need different resources, the modules, and parts of modules, from the CUSP Toolkit can be used independently and presented in whatever circumstances are most appropriate for the user's needs. We encourage all users to review the introductory materials and skim through the entire toolkit before finalizing decisions about how best to use the information.
Materials in this toolkit come from several general sources, including:
- Resources and content developed to support the Keystone CLABSI initiative in Michigan and the subsequent AHRQ-funded national project.
- AHRQ materials that address teamwork and culture and use quality-improvement data that align, complement, and enhance the resources crafted for the AHRQ-funded national project.
- Original resources, such as exercises, illustrations, and video vignettes, to assist organizations that did not participate in the national project, to ensure alignment with other initiatives that are currently underway in organizations, and to provide the most comprehensive set of safety resources to users.
[D] Select for Text Description.
Slide 13. Toolkit Users
Senior executives, Patient safety officers, and Nurse managers.
Say:
Anyone can employ the CUSP Toolkit. People across an organization and team members of any discipline or rank can use the toolkit and expect measurable results.
The toolkit can be used by:
- Senior executives.
- Patient safety officers.
- Nurse managers.
- Frontline staff.
- Physician champions.
Senior executives
The toolkit can help senior leaders prioritize improvement efforts and administer resources for interventions to alleviate defects. After a team has identified safety-related defects in their unit and has determined their root causes, resources to address them often need senior leadership approval. Senior executives can work across the organization to help remove departmental barriers to safety. Greater familiarity with the CUSP model can offer senior leaders the context necessary to make informed decisions about the competing demands for resources.
Patient safety officers
Patient safety officers can use the toolkit when working with senior executives and unit managers to maintain an ongoing infrastructure for improvement activities and to assist with organization-wide spread of unit improvement work.
Nurse managers
As unit leaders, nurse managers have the ability to communicate with leaders, reallocate resources, serve on teams, and be role models for change. Nurse managers can incorporate the CUSP Toolkit to educate their teams about the science of safety and provide opportunities for staff to learn and practice using teamwork and communication tools. The videos in the "Understand the Science of Safety" module articulate the importance of seeing defects in care, not only in terms of actions or attitudes of individual care providers but also in terms of systems of care.
[D] Select for Text Description.
Slide 14. Toolkit Users
Frontline staff: Engage with Stakeholders in safety improvement. Physician champions: Share knowledge on the immediate and long-term benefits of teamwork and communication tools.
Say:
Frontline staff
There are actually two sets of activities that take place in any health care unit: activities of care delivery and activities to improve patient care. Sustainable improvement can occur when frontline staff members take ownership of the improvement process. Frontline staff can use the modules to educate one another, patients, and physicians. They can further use communication tools to engage with physicians, patients, and staff in other disciplines or departments.
Physician champions
Physician champions, who support teamwork and communication improvements and take a leadership role, can apply the toolkit to share knowledge about the immediate and long-term benefits of teamwork and communication tools. The toolkit can also be used with other disciplines and departments, such as pharmacy, laboratory, quality improvement, admissions, and health information management.
[D] Select for Text Description.
Slide 15. Implementation

Say:
There are many ways to use the CUSP Toolkit. Users can:
- Share videos with teams to spark engagement and learning.
- Provide templates and discussion guides to project leads.
- Educate teams about the science of safety.
- Use videos and training modules to orient new clinical staff.
- Train teams to use teamwork and communication tools.
- Engage senior executives and physician champions.
Each module in the CUSP Toolkit includes video vignettes, which can be powerful mechanisms to spark the engagement of frontline providers in the unit. Furthermore, communication templates and vital information about the science of safety can empower teams to examine defects in care with respect to systems and to address root causes of defects more effectively.
The "Implement Teamwork and Communication" module presents a number of useful structured communication tools, including resources from TeamSTEPPS. The resources in that module will help unit teams prevent misunderstandings and improve teamwork, the most significant contributing factors identified to prevent patient harm or errors in care.
Tools such as clinician shadowing and the Staff Safety Assessment can be particularly effective in engaging senior executives and physician champions by demonstrating the need for executive and physician involvement and safety improvement.
[D] Select for Text Description.
Slide 16. Challenges
. Senior executive engagement and participation. High staff turnover. Nurse empowerment.")
Say:
Users may encounter challenges when making use of the toolkit, such as:
- Modifying CUSP to meet the needs of specialty units, such as neonatal ICUs, oncology, dialysis, and burn units.
- Engaging the interest and participation of senior executives.
- Contending with high staff turnover.
- Ensuring nurse empowerment.
These kinds of issues will make CUSP implementation both more challenging and more necessary.
Needs of specialty units vary from the typical ICU. For example, care workflows can vary drastically in units such as those in neonatal ICUs, oncology, and dialysis, as well as in burn units. If CUSP implementation stalls in these units, focused use of the Staff Safety Assessment tool, which is introduced in the "Identify Defects Through Sensemaking" module, can provide a point of entry. The Staff Safety Assessment asks two key questions of teams:
- How might the next patient be harmed in our unit?
- What can be done to minimize the risk of harm?
This assessment will help users access the knowledge at the front lines of patient care to determine what risks are present in the unit.
In other implementations of CUSP, senior executive buy-in might be the most substantial challenge a team faces. Engaging senior executives who do not have a clinical background is particularly challenging. In these situations the use of a tool like an Opportunity Estimator, which calculates estimated lives lost and dollars spent as the result of CLABSIs, can engage hospital executives with the prospective cost savings that can result from CUSP implementation. An Opportunity Estimator uses data from the total number central-line days, percentage of case fatalities, total number of incidents, and cost per infection to determine the overall savings that can be achieved through CUSP procedures. Encouraging senior executives, particularly those without a clinical background, to shadow a nurse or physician champion can help them to better understand unit challenges firsthand.
High staff turnover also poses major challenges to CUSP implementation. High turnover adversely affects the amount and quality of training team members receive. Focused use of the "Understand the Science of Safety" module can provide a necessary primer on the concepts used in CUSP tools and other modules of the toolkit.
Nurse empowerment can also be a concern for some teams. In these cases, using role-play exercises during training sessions allows nurses to practice speaking up and helps them to gain confidence in addressing situations with noncompliant physicians. Distributing pocket cards with information on necessary improvement areas, such as unit infection rates, can also provide impetus for them to speak up in situations with other members of the health care team.
[D] Select for Text Description.
Slide 17. Assemble the Team

Say:
There are four learning objectives in the "Assemble the Team" module:
- Understand the importance of your CUSP team.
- Develop a strategy to build a successful team.
- Identify characteristics of effective teams and barriers to team performance.
- Define roles and responsibilities of team members.
[D] Select for Text Description.
Slide 18. Barriers to Team Performance3

Say:
Barriers to team performance include:
- Inconsistency in team membership.
- Lack of time and information sharing.
- Hierarchy.
- Varying communication styles.
- Presence of conflict.
- Lack of coordination and follow-up.
- Misinterpretation of cues.
- Lack of role clarity.
CUSP and TeamSTEPPS identify similar barriers to team performance. Inconsistency in team membership hampers performance by limiting the strength and resiliency of the unit team. Teams that lack sufficient structure, with inconsistent input, or that lack fully engaged members, will encounter difficulties with their team performance. Teams that do not, or are unable to, devote the necessary time and energy for the initiative will also run into challenges with functionality. Information should be shared equally among unit team members.
Hierarchy may hinder unit team success by limiting opportunities for communication and interaction. If team members feel intimidated, the initiative's effectiveness will be diminished.
Additional barriers to successful teamwork include conflict, lack of coordination, misinterpretation of cues, and lack of role clarity. Disputes are common in groups with diverse opinions, but conflict resolution and team interaction will help strengthen the initiative. Maintaining clear roles and task coordination are also key and will alleviate task or labor duplication, further assisting with the success of the initiative.
[D] Select for Text Description.
Slide 19. Engage the Senior Executive
Text Description is below the image. Image: Two senior executives standing next to each other.
Say:
The four learning objectives from the "Engage the Senior Executive" module are:
- Identify characteristics to search for when recruiting the senior executive.
- Describe the responsibilities of the senior executive.
- Explain the role of the senior executive in addressing technical and adaptive work.
- Explain how to engage the senior executive and develop shared accountability for the work.
[D] Select for Text Description.
Slide 20. The Challenges of Partnering with a Senior Executive

Say:
When engaging the proposed senior executive member of the CUSP team, the team's progress may be challenged because the senior executive:
- May lack clinical background.
- May not recognize the value of CUSP.
- May not be able to meet with the CUSP team regularly.
These hurdles are external. Many executives can be effectively engaged with the proper technique. Through following the 4 E's Engagement Model, which is explained in the "Assemble the Team" module, CUSP teams will be able to customize their appeal and project approach to meet the needs and clinical background of their executive partner.
When senior executives cite their lack of a clinical background, unit team members can focus their appeal on the fiscal gains associated with patient safety initiatives. If executives are unable to see the value of CUSP for the unit or the hospital, unit team members should relate success stories or real data that highlight the triumphs other unit teams have experienced when implementing CUSP initiatives in their units. If executives claim a busy schedule as a barrier to involvement in the project, the team can arrange monthly meetings via conference calls.
Ask:
What barriers do you foresee in appointing a hospital executive to serve as your team member?
[D] Select for Text Description.
Slide 21. Understand the Science of Safety

Say:
In the "Understand the Science of Safety" module, the four primary learning objectives are:
- Describe the historical and contemporary context of the Science of Safety.
- Explain how system design affects system results.
- List the principles of safe design and identify how they apply to technical work and teamwork.
- Indicate how teams make wise decisions when there is diverse and independent input.
[D] Select for Text Description.
Slide 22. System-Level Factors Impact Safety5

Say:
At any given time, there are several system factors that simultaneously influence unit culture and patient safety.
One factor is patient characteristics.
Patient characteristics, such as medical history, acuity, primary language, or ability to participate in the development of the care plan can influence patient safety.
Relevant to those are task factors.
In addition to patient characteristics, task factors can shape the delivery of care and patient safety in the unit. Patient complexity influences both providers' ability to meet patient needs and their capacity to manage the task of care.
The individual provider is another system factor.
Providers should understand the relationship between their own knowledge, skill, and attitudes, and how these may benefit or detract from the quality of care that patients receive. Providers should be comfortable speaking up if they are not in agreement with task assignments and protocols or when they see patient safety risks. Evidence suggests a direct relationship between some patient outcomes and the willingness of staff to speak up.
Team factors are equally important.
Team factors may involve issues with teamwork, communication, inadequate supervision, and training.
The work environment can be a major factor.
Noisy, dirty, distracting, and poorly lit work environments can wreak havoc on the delivery of high-quality patient care and should be addressed when attempting to diagnose system-level influences on patient care.
Besides unit factors, there are departmental factors.
When staffing issues, admission policies, and protocols prove to be insufficient for the needs of the patient and provider, they will affect the quality of care. Staffing and coverage shortages cause patients to suffer through missing the attention necessary to recover. Additionally, staffing and coverage issues can increase the likelihood for medication or health care procedure errors, downgrading the type of care patients receive.
And last are hospital and institutional factors.
The type of facility and budget limitations may adjust a patient's care plan. While these factors are the furthest removed from the patient, they continually alter care delivered during hospital recovery.
[D] Select for Text Description.
Slide 23. Identify Defects Through Sensemaking

Say:
The four learning objectives for the "Identify Defects Through Sensemaking" module are:
- Introduce CUSP and Sensemaking tools to identify defects and errors.
- Discuss the relationship between CUSP and Sensemaking.
- Show how to apply CUSP and Sensemaking tools.
- Discuss how to share findings.
Note: This module combines the CUSP steps Identify Defects and Learn from Defects.
[D] Select for Text Description.
Slide 24. Examples of Defects or Errors That Affect Patient Safety

Say:
When identifying defects that affect patient care, knowing how a defect will affect patient safety can help the team prevent the defect as well as a sentinel event. In doing this, providers understand the relationship between production pressures and defects in the health care system in addition to the intended outcomes that these can produce.
Examples of defects or errors that affect patient safety, and the interventions to alleviate them include:
- Unstable oxygen tanks on beds: oxygen tank holders were repaired or new holders were installed institution-wide.
- Medication look-alikes: Staff were educated about medication similarities, physical separation of medications was instituted, and a letter was sent to the manufacturer to request different labeling.
- Missing equipment on the cart: A checklist was developed for assigning responsibility for stocking supplies on the cart.
- Inconsistent use of Daily Goals Rounding Tool: A consensus was reached among staff on the elements of the tool to be applied during rounds.
- Residents' use of inaccurate information during rounds: Electronic progress notes were developed to maintain accurate information exchanges on the unit.
[D] Select for Text Description.
Slide 25. Implement Teamwork and Communication

Say:
The "Implement Teamwork and Communication" module covers these four learning objectives:
- Recognize the importance of effective communication.
- Identify barriers to communication.
- Describe the connection between communication and medical error.
- Identify and apply effective communication strategies from CUSP and TeamSTEPPS.
[D] Select for Text Description.
Slide 26. Elements That Affect Communication and Information Exchange

Say:
Communication problems are cited as the root cause of most errors in studies by the Joint Commission and others. Several elements affect communication and information exchange, such as:
- Interruptions, which limit the ability of team members to discuss and comprehend necessary information.
- Task absorption, which reduces focus of unit team efforts on other necessary tasks.
- Verbal abuse, which creates a hostile environment in which team members do not feel comfortable sharing ideas or collaborating to solve an issue at hand.
- Fatigue, which decreases the level of attention and energy that team members are able to devote to the project.
- Not following the plan of care, which lowers the effectiveness of planned interventions and activities.
- Ambiguous orders or directions, which cloud expectations and plans.
- Change in team members, which strains existing work relationships between established unit team members and the newest additions to the unit team.
- Heavy workloads, which hinder clear communication.
[D] Select for Text Description.
Slide 27. Apply CUSP

Say:
The three "Apply CUSP" learning objectives are:
- Introduce Just Culture principles.
- Learn how Just Culture principles can augment CUSP.
- Review key steps of the CUSP Toolkit.
A Just Culture learning environment allows the review of both system design and the employee's choice of behavior in response to assigned duties. It provides a comprehensive process to investigate harmful events or patient safety concerns and determine an appropriate course of action with the employees involved.
Just Culture principles are a crucial accompaniment to the CUSP framework and will spark the shared accountability that is necessary for CUSP implementation to be successful. David Marx developed the Just Culture framework based on risk management concepts from high-reliability industries, such as aviation and nuclear energy.
A Just Culture is a system that holds itself accountable, holds staff members accountable, and has staff members who hold themselves accountable. Shared responsibility is the norm in a Just Culture, and a commitment to eliminating the possibility of error is widespread within a Just Culture.
[D] Select for Text Description.
Slide 28. The CUSP Model Generates Measurable Results7
 to 52.2 percent (2006). In 2009, more than 350 hospitals in 22 States reduced CLABSI rates by an average of 35 percent after implementing CUSP.")
Say:
The CUSP model generates measurable results. The CUSP implementation in the Michigan Keystone ICU Project was correlated with considerable improvements in the safety climate in 71 units, as measured by a unit culture survey. Overall mean safety climate scores significantly improved from 42.5 percent in 2004 to 52.2 percent in 2006.
CUSP implementation and the improvements in workplace culture that it brings also make technical improvements in care possible. In 2009, more than 350 hospitals in 22 States reduced CLABSI rates by an average of 35 percent. All of these units implemented CUSP, and many continue to see rates at or near zero over extended time.
[D] Select for Text Description.
Slide 29. CUSP Results

Say:
Culture change is hard work. As you complete the adaptive work of improving patient safety and confront challenges that will seem messy and intractable, keep your eyes on the prize and remember that in thousands of units all over the country, CUSP has brought measurable results. CUSP will help unit teams achieve:
- Heightened engagement of staff and senior leaders.
- Improved communication among care team members.
- Shared mental models.
- Expanded knowledge of potential hazards and barriers to safety.
- Collaborative focus on systems of care.
[D] Select for Text Description.
Slide 30. Summary

Say:
CUSP integrates with and supports a broad range of quality and safety improvement models. As teams use CUSP and its tools, they should look at resources already in place and enhance the projects by combining them in efficient and effective ways.
People across an organization, and team members of any discipline or rank, can use the CUSP Toolkit and expect measurable results.
Any implementation of CUSP will bring with it certain challenges. In confronting these challenges, often concentration on a specific module or tool in the CUSP Toolkit will help overcome obstacles. For example, the Staff Safety Assessment can help to pinpoint the particular needs of specialty units, and the Shadowing Another Professional tool can trigger greater participation from your senior executive partner and physician champion.
CUSP is an investment in time, energy, and dedication that brings both tangible and intangible benefits. When CUSP tools become integrated into routine daily and weekly workflows, the process of improving safety will become a recognized complement to the process of care delivery itself. CUSP implementation can lead to improved safety and improved staff satisfaction and retention.
[D] Select for Text Description.
Slide 31. References

[D] Select for Text Description.
Slide 32. References

[D] Select for Text Description.