

Chartbook on Hispanic Health Care: Slide Presentation
2014 National Healthcare Quality and Disparities Report
Contents
Introduction
Part 1: Overviews of the Report and the Hispanic Population
Part 2: Trends in Priorities of the Heckler Report
Part 3: Trends in Access and Priorities of the National Quality Strategy
Part 4: Health Care of Residents of the U.S.-Mexico Border
Introduction
Slide 1
National Healthcare Quality and Disparities Report
Chartbook on Health Care for Hispanics
October 2015
Slide 2
Goals of the Chartbook on Health Care for Hispanics
- Commemorates the 30th Anniversary of the Report of the Secretary's Task Force on Black and Minority Health (Heckler Report).
- Highlights progress for Hispanics on priorities of the Heckler Report.
- Summarizes trends in health care disparities by Hispanic ethnicity related to:
- Access to health care.
- Priorities of the National Quality Strategy (NQS).
- Presents information on a unique, largely Hispanic population: residents of the U.S.-Mexico border.
Slide 3
Organization of the Chartbook on Health Care for Hispanics
- Part of a series related to the National Healthcare Quality and Disparities Report (QDR).
- Organized into four parts:
- Overviews of the QDR and the Hispanic population, one of AHRQ's priority populations.
- Summary of trends in health care for Hispanic populations related to priorities of the Heckler Report.
- Summary of trends in health care for Hispanic populations related to access to health care and NQS priorities.
- Information on health care received by residents of the U.S.-Mexico border, a unique and largely Hispanic population.
Slide 4
Key Findings of the Chartbook on Health Care for Hispanics
- Data on access to and quality of health care received by Hispanics were available for almost all measures tracked in the QDR.
- Among Heckler Report priorities, disparities in mental health care and diabetes care were big problems for Hispanics.
- Hispanics have worse access to care although this is improving since the Affordable Care Act.
- Hispanics receive poorer quality of care, especially as related to person centeredness.
- Residents of the U.S.-Mexico border face unique health care challenges.
Part 1: Overviews of the Report and the Hispanic Population
Slide 5
National Healthcare Quality and Disparities Report Chartbook on Health Care for Hispanics
Part 1:Overviews of the Report and the Hispanic Population
Slide 6
National Healthcare Quality and Disparities Report
- Annual report to Congress mandated in the Healthcare Research and Quality Act of 1999 (P.L. 106-129).
- Provides a comprehensive overview of:
- Quality of health care received by the general U.S. population.
- Disparities in care experienced by different racial, ethnic, and socioeconomic groups.
- Assesses the performance of our health system and identifies areas of strengths and weaknesses along three main themes:
- Access to health care.
- Quality of health care.
- NQS priorities.
Slide 7
National Healthcare Quality and Disparities Report
- Based on more than 250 measures of quality and disparities covering a broad array of health care services and settings.
- Data generally available through 2012.
- Produced with the help of an Interagency Work Group led by the Agency for Healthcare Research and Quality and submitted on behalf of the Secretary of Health and Human Services.
Slide 8

Key Findings of the 2014 QDR
- The Nation has made clear progress in improving the health care delivery system to achieve the three aims of better care, smarter spending, and healthier people.
- There is still more work to do, specifically to address disparities in care.
- Access improved.
- Quality improved for most National Quality Strategy priorities.
- Few disparities were eliminated.
- Many challenges in improving quality and reducing disparities remain.
Slide 9
Chartbook on Health Care for Hispanics
- This chartbook includes summaries of trends in health care for Hispanic populations related to:
- Priorities of the Heckler Report.
- Access to health care.
- Priorities of the National Quality Strategy.
- Introduction and Methods contains information about methods used in the chartbook.
- Appendixes include information about measures and data.
- A Data Query tool (http://nhqrnet.ahrq.gov/inhqrdr/data/query) provides access to all data tables.
Slide 10
Key Metrics Used in Chartbooks
- Trends: Assesses the rate of change over time (typically 2002-2012) for a population using regression for measures with 4+ time points.
- Disparities: Assesses whether measure estimates for two populations differ at the most recent time point.
- Change in Disparities: Assesses whether the rates of change over time for two populations differ using regression.
- Achievable Benchmarks: Defines a level of performance for a measure that has been attained by the best performing States.
Note:
- In this chartbook Hispanics are usually contrasted with non-Hispanic Whites and non-Hispanic Blacks. To make text more concise, the labels White and Black are used to refer to populations that are non-Hispanic White and non-Hispanic Black, respectively. In addition, unless otherwise specified, Hispanics include all races.
- Examples of successful interventions come from the AHRQ Health Care Innovations Exchange: https://innovations.ahrq.gov/.
- Go to Introduction and Methods for more information about methods used in the chartbook.
Slide 11
HHS Data Collection Standards for Race and Ethnicity, 2011
Note:
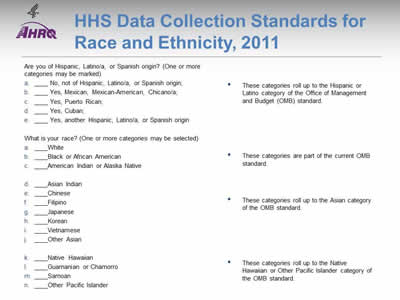
- The Affordable Care Act includes several provisions aimed at eliminating health disparities in America. Section 4302 (Understanding health disparities: data collection and analysis) focuses on the standardization, collection, analysis, and reporting of health disparities data. Section 4302 requires the Secretary of Health and Human Services (HHS) to establish data collection standards for race, ethnicity, sex, primary language, and disability status. Adopted October 31, 2011, these data collection standards are to be used, to the extent practicable, in HHS-sponsored population health surveys.
- The new data standards improve the quality of HHS data collection by establishing a consistent, uniform way to capture, record, and report data on race and ethnicity with additional granularity (beyond the OMB minimum) for the Asian race category and Hispanic ethnicity, and for the first time, standardized collection of language and disability status data.
- Because many of the data available to produce this chartbook were collected in 2012 and earlier, there was insufficient time to incorporate the new 2011 standards . Thus, much of the information presented here will show estimates for Hispanics in aggregate. For several data sources, information was collected for more granular Hispanic groups, and this is presented to illustrate the importance of collecting this more granular information.
Slide 12
Diversity of the Hispanic Population in the United States
- Hispanics in the United States are a diverse population, including:
- Mexicans (64%).
- Puerto Ricans (9.4%).
- Cubans (3.7%).
- South Americans (5.9%).
- Central Americans (9%).
- Other Spanish origin groups.
- Although socioeconomically disadvantaged (except Cubans), Hispanics, particularly Mexican women, have better mortality rates than Whites.
Note:
Slide 13
Health of the Hispanic Population in the United States
- Health of Hispanics is influenced by many factors, including language, lack of access to preventive care, lack of health insurance, and other cultural barriers.
- Leading causes of morbidity and mortality include heart disease, cancer, unintentional injuries, stroke, and diabetes.
- Compared with non-Hispanic Whites, Hispanics have a:
- Higher prevalence of asthma, chronic obstructive pulmonary disease, HIV/AIDS, suicide, and liver disease.
- Higher rate of obesity.
Note:
Slide 14
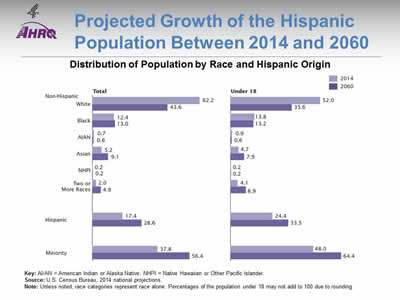
Projected Growth of the Hispanic Population Between 2014 and 2060
Distribution of Population by Race and Hispanic Origin
Image: Two bar charts compare distribution of population by race for 2014 and projected for 2060. Total: White, 2014 - 62.2%; White, 2060 - 43.6%. Black, 2014 - 12.4%; Black, 2060 - 13.0%. AIAN, 2014 - 0.7%; AIAN, 2060 - 0.6%. Asian, 2014 - 5.2%; Asian, 2060 - 9.1%. NHPI, 2014 - 0.2%; NHPI, 2060 - 0.2%. Two or More Races, 2014 - 2.0%; Two or More Races, 2060 - 4.9%. Hispanic, 2014 - 17.4%; Hispanic, 2060 - 28.6%. Minority, 2014 - 37.8%; Minority, 2060 - 56.4%. Under 18: White, 2014 - 52.0%; White, 2060 - 35.6%. Black, 2014 - 13.8%; Black, 2060 - 13.2%. AIAN, 2014 - 0.9%; AIAN, 2060 - 0.6%. Asian, 2014 - 4.7%; Asian, 2060 - 7.9%. NHPI, 2014 - 0.2%; NHPI, 2060 - 0.2%. Two or More Races, 2014 - 4.1%; Two or More Races, 2060 - 8.9%. Hispanic, 2014 - 24.4%; Hispanic, 2060 - 33.5%. Minority, 2014 - 48.0%; Minority, 2060 - 64.4%.
Key: AI/AN = American Indian or Alaska Native; NHPI = Native Hawaiian or Other Pacific Islander.
Source: U.S. Census Bureau, 2014 national projections.
Note: Unless noted, race categories represent race alone. Percentages of the population under 18 may not add to 100 due to rounding.
- In 2060, it is projected that 28.6% of the total U.S. population and 33.5% of U.S. children will be Hispanic.
Slide 15
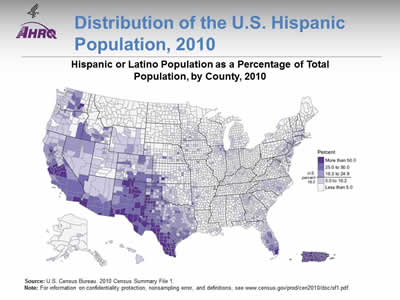
Distribution of the U.S. Hispanic Population, 2010
Hispanic or Latino Population as a Percentage of Total Population, by County, 2010
Image: A map of the United States is color-coded by county to show percentage of Hispanic or Latino Population.
Source: U.S. Census Bureau. 2010 Census Summary File 1.
Note: For information on confidentiality protection, nonsampling error, and definitions, go to http://www.census.gov/prod/cen2010/doc/sf1.pdf (7.384 MB).
- Hispanics are concentrated in specific geographic locations. Three quarters of the U.S. Hispanic population live in eight States:
- California (28% of Hispanics in the United States).
- Texas (19%).
- Florida (8%).
- New York (7%).
- Illinois (4%).
- Arizona (4%).
- New Jersey (3%).
- Colorado (2%).
- One-quarter of the U.S. Hispanic population live in eight counties:
- 4.7 million Hispanics in Los Angeles County, California.
- 1.7 million in Harris County, Texas.
- 1.6 million in Miami-Dade County, Florida.
- 1.2 million in Cook County, Illinois.
- 1.1 million in Maricopa County, Arizona.
- 1.0 million in each of the following counties: Orange, California; Bexar, Texas; and San Bernardino, California.
Slide 16
Hispanic Mothers and Children
- About 84% of Hispanic mothers receive early prenatal care compared with 87% of White mothers.
- Most Hispanic populations have lower infant mortality rates than Whites.
- Infant mortality rates range from 3.0 for Cuban Americans to 5.9 for Puerto Ricans compared with 5.1 for non-Hispanic Whites.
- Congenital malformation, low birthweight, and maternal complications are the leading causes of infant mortality among Hispanics.
Note:
- Source: https://www.acog.org; Markides & Coreil, 1986; http://minorityhealth.hhs.gov.
Slide 17
Older Hispanics in the United States
- In 2012, there were:
- 3.1 million Hispanics age 65 and over (7% of older adults); by 2060, this is projected to increase to more than 19 million, accounting for 21% of older adults.
- 4,129 Hispanics age 100 and over (1,105 men, 3,024 women), or 7% of all centenarians.
- Most (70%) older Hispanics lived in four States: California, Texas, Florida, and New York.
Note:
Slide 18
Health of Older Hispanics in the United States
- In 2012, the top five chronic conditions among older Hispanics were hypertension, arthritis, heart disease, diabetes, and cancer.
- Nearly one-quarter (24%) of older Hispanics had Medicare and supplementary private health insurance compared with 50% of all older adults.
- Nearly one-quarter (23%) of older Hispanics were covered by Medicare and Medicaid compared with 8% of all older adults.
Note:
Part 2: Trends in Priorities of the Heckler Report
Slide 19
National Healthcare Quality and Disparities Report Chartbook on Health Care for Hispanics
Part 2: Trends in Priorities of the Heckler Report
Slide 20
Report of the Secretary's Task Force on Black and Minority Health (Heckler Report)
- 30th anniversary of the Heckler Report, released in 1985 under the leadership of then U.S. Department of Health and Human Services Secretary Margaret M. Heckler.
- Documented persistent health disparities that accounted for 60,000 excess deaths each year.
Note:
- This year marks the 30th anniversary of the Report of the Secretary's Task Force on Black and Minority Health (also known as the Heckler Report), released in 1985 under the leadership of then U.S. Department of Health and Human Services (HHS) Secretary Margaret M. Heckler. The landmark report marked the first convening of a group of health experts by the U.S. government to conduct a comprehensive study of racial and ethnic minority health and elevated minority health onto a national stage.
- The Heckler Report documented persistent health disparities that accounted for 60,000 excess deaths each year and synthesized ways to advance health equity. This marked the beginning of a new era in addressing minority health issues, beginning with the creation of the HHS Office of Minority Health in 1986 and leading up to the Affordable Care Act in 2010.
Slide 21
Priorities of the Heckler Report
- Focused on six causes of death with large Black-White disparities:
- Cancer.
- Cardiovascular disease and stroke.
- Chemical dependency.
- Diabetes.
- Homicide and accidents.
- Infant mortality.
- Data on "other minorities," including Hispanics:
- Very limited in the 1980s.
- Much more available today.
Note:
- The Heckler Report found that 6 causes of death accounted for more than 80% of mortality among Blacks and other minority groups compared with Whites. These include cancer; cardiovascular disease and stroke; chemical dependency (measured by deaths due to cirrhosis); diabetes; homicide and accidents (unintentional injuries); and infant mortality. Based on the findings, the report outlined recommendations in areas of urgent need, including health information and education; health services delivery and financing; health professions development; data development; and research agenda.
- With the rapidly increasing diversity of the Nation and persistence of health disparities, the Heckler Report 30th anniversary serves as a call for all Americans to take action and accelerate efforts toward ending health disparities and achieving health equity in their community.
Slide 22
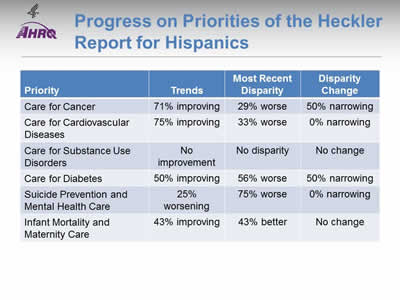
Progress on Priorities of the Heckler Report for Hispanics
| Priority | Trends | Most Recent Disparity | Disparity Change |
|---|---|---|---|
| Care for Cancer | 71% improving | 29% worse | 50% narrowing |
| Care for Cardiovascular Diseases | 75% improving | 33% worse | 0% narrowing |
| Care for Substance Use Disorders | No improvement | No disparity | No change |
| Care for Diabetes | 50% improving | 56% worse | 50% narrowing |
| Suicide Prevention and Mental Health Care | 25% worsening | 75% worse | 0% narrowing |
| Infant Mortality and Maternity Care | 43% improving | 43% better | No change |
Note:
- Trends:
- Most measures of care for cancer and care for cardiovascular diseases were improving for Hispanics.
- About half of measures for diabetes care and maternity care were improving.
- No measures of care for substance use disorders were improving and mental health care seemed to be getting worse for Hispanics.
- Groups With Disparities:
- For many measures of care for mental health disorders, diabetes, cardiovascular diseases, and cancer, Hispanics received worse quality of care than non-Hispanic Whites. Hispanics tended to receive better quality of maternity care.
- Of measures for which Hispanics received worse quality of care than non-Hispanic Whites, narrowing of the gap was observed for several measures of cancer and diabetes care. No narrowing of disparities was observed among measures of cardiovascular and mental health care.
- Summary: Of priorities of the Heckler Report:
- Suicide prevention and mental health care for Hispanics is worsening, with many disparities and no reductions in disparities over time.
- Hispanics also experience many disparities in care for diabetes.
- Care for substance use disorders is poor for all ethnic groups.
Slide 23

National Healthcare Quality and Disparities Report Chartbook on Health Care for Hispanics
Part 2: Trends in Priorities of the Heckler Report
Care for Cancer
Note:
- Thirty years ago, the Heckler Report found that:
- Overall age-adjusted cancer incidence rates for Hispanics were lower than for Blacks or nonminorities. Specific sites of excess incidence among Hispanics were the stomach, prostate, esophagus, pancreas, and cervix.
- The overall 5-year relative survival rate of Hispanic males was almost identical to that of nonminorities. Hispanic females had somewhat lower survival rates than nonminority females.
- Mortality data are derived from the National Center for Health Statistics (NCHS) through the vital statistics system. This system classifies Hispanics as Whites, so no death statistics on Hispanics are presented.
- Today, death statistics on Hispanics are available. In addition, quality care for cancer has changed. Evidence-based mass screening is recommended in specific populations for four cancers: breast, cervical, colorectal, and lung cancer. Screening is the first step in the process of cancer prevention (Pap testing for cervical and colonoscopy for colorectal) and early detection (mammography for breast and CT scan for lung) in the process of cancer control. Hence, screenable cancers have been selected for inclusion in this chartbook.
Slide 24
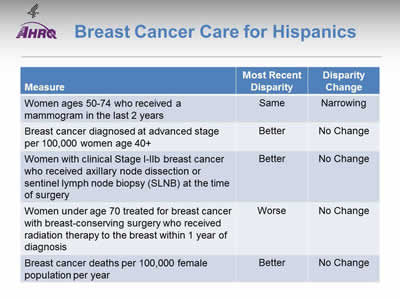
Breast Cancer Care for Hispanics
| Measure | Most Recent Disparity | Disparity Change |
|---|---|---|
| Women ages 50-74 who received a mammogram in the last 2 years | Same | Narrowing |
| Breast cancer diagnosed at advanced stage per 100,000 women age 40+ | Better | No Change |
| Women with clinical Stage I-IIb breast cancer who received axillary node dissection or sentinel lymph node biopsy (SLNB) at the time of surgery | Better | No Change |
| Women under age 70 treated for breast cancer with breast-conserving surgery who received radiation therapy to the breast within 1 year of diagnosis | Worse | No Change |
| Breast cancer deaths per 100,000 female population per year | Better | No Change |
Note:
- Trends: Most measures of breast cancer care for Hispanics were improving.
- Groups With Disparities:
- Rates of mammography were similar between Hispanic and White women. This represents the elimination of a previously observed disparity.
- Rates of diagnosis with advanced stage breast cancer and death due to breast cancer were lower among Hispanics compared with non-Hispanic Whites and these disparities were not changing over time.
- Hispanic women were more likely to receive axillary node dissection at time of surgery and this disparity did not change over time.
- Hispanics were less likely to receive radiation therapy after breast-conserving surgery compared with Whites. This disparity did not change over time.
Slide 25
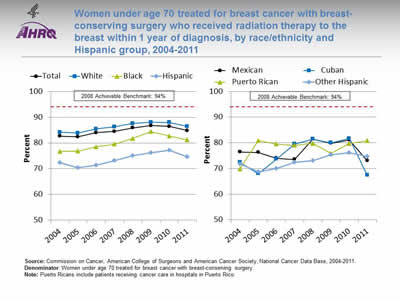
Women under age 70 treated for breast cancer with breast-conserving surgery who received radiation therapy to the breast within 1 year of diagnosis, by race/ethnicity and Hispanic group, 2004-2011
Image: Graphs show women under age 70 treated for breast cancer with breast-conserving surgery who received radiation therapy to the breast within 1 year of diagnosis:
Left Graph:
| Race/Ethnicity | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 |
|---|---|---|---|---|---|---|---|---|
| Total | 82.6 | 82.4 | 84.0 | 84.5 | 85.9 | 86.7 | 86.4 | 84.8 |
| White | 84.2 | 83.8 | 85.5 | 86.2 | 87.6 | 88.1 | 88.0 | 86.4 |
| Black | 76.7 | 76.8 | 78.6 | 79.6 | 81.7 | 84.4 | 82.7 | 81.2 |
| Hispanic | 72.3 | 70.5 | 71.4 | 73.2 | 75.1 | 76.2 | 77.2 | 74.6 |
2008 Achievable Benchmark: 94%.
Right Graph:
| Hispanic Group | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 |
|---|---|---|---|---|---|---|---|---|
| Mexican | 76.4 | 76.3 | 74.0 | 73.5 | 81.5 | 79.8 | 81.1 | 73.0 |
| Cuban | 72.4 | 68.0 | 73.7 | 79.5 | 81.5 | 80.0 | 81.7 | 67.4 |
| Puerto Rican | 69.9 | 80.9 | 79.5 | 79.0 | 79.7 | 75.9 | 79.8 | 80.8 |
| Other Hispanic | 71.8 | 68.6 | 70.1 | 72.4 | 73.1 | 75.4 | 76.2 | 74.6 |
2008 Achievable Benchmark: 94%.
Source: Commission on Cancer, American College of Surgeons and American Cancer Society, National Cancer Data Base, 2004-2011.
Denominator: Women under age 70 treated for breast cancer with breast-conserving surgery.
Note: Puerto Ricans include patients receiving cancer care in hospitals in Puerto Rico.
- Importance: Radiation therapy after breast-conserving surgery reduces the risk of cancer recurrence and death.
- Trends: From 2004 to 2011, the percentage of women with breast-conserving surgery who received radiation therapy to the breast improved overall and among all racial/ethnic groups.
- Groups With Disparities:
- In all years, Hispanic and Black women were less likely to receive radiation therapy to the breast compared with White women.
- In all years, Mexicans and other Hispanics were also less likely to receive radiation therapy to the breast compared with White women.
- Achievable Benchmark:
- The 2008 top 5 State achievable benchmark was 94%. The top 5 States that contributed to the achievable benchmark are Kansas, Minnesota, Montana, North Dakota, and Wisconsin.
- At the current rates of improvement, the benchmark could not be achieved overall for about 17 years.
- At the current rates of improvement, Whites would need 14 years to achieve the benchmark, and Hispanics would need 25 years.
Slide 26
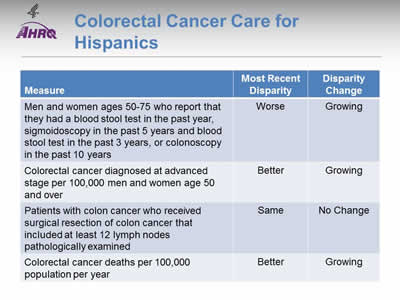
Colorectal Cancer Care for Hispanics
| Measure | Most Recent Disparity | Disparity Change |
|---|---|---|
| Men and women ages 50-75 who report that they had a blood stool test in the past year, sigmoidoscopy in the past 5 years and blood stool test in the past 3 years, or colonoscopy in the past 10 years | Worse | Growing |
| Colorectal cancer diagnosed at advanced stage per 100,000 men and women age 50 and over | Better | Growing |
| Patients with colon cancer who received surgical resection of colon cancer that included at least 12 lymph nodes pathologically examined | Same | No Change |
| Colorectal cancer deaths per 100,000 population per year | Better | Growing |
Note:
- Trends: All measures of colorectal cancer care for Hispanics were improving.
- Groups With Disparities:
- Hispanics were less likely to receive colorectal cancer screening than Whites and this disparity was growing over time.
- Rates of diagnosis with advanced stage colorectal cancer and death due to colorectal cancer were lower among Hispanics compared with Whites. These disparities were growing over time.
- Rates of surgical resection of colon cancer that included at least 12 lymph nodes pathologically examined were similar between Hispanics and Whites.
Slide 27
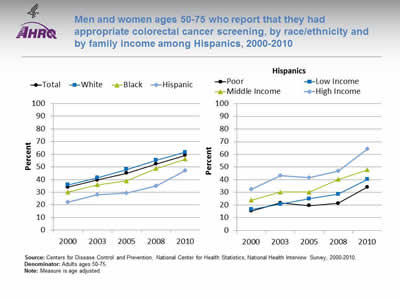
Men and women ages 50-75 who report that they had appropriate colorectal cancer screening, by race/ethnicity and by family income among Hispanics, 2000-2010
Image: Graphs show men and women ages 50-75 who report that they had appropriate colorectal cancer screening:
Left Graph:
| Race/Ethnicity | 2000 | 2003 | 2005 | 2008 | 2010 |
|---|---|---|---|---|---|
| Total | 34.1 | 39.6 | 45.0 | 52.2 | 59.2 |
| Hispanic | 22.0 | 28.1 | 29.3 | 35.0 | 47.2 |
| Black | 30.1 | 35.9 | 39.0 | 48.7 | 56.2 |
| White | 35.8 | 41.4 | 48.0 | 55.2 | 61.6 |
Right Graph (Hispanics):
| Income | 2000 | 2003 | 2005 | 2008 | 2010 |
|---|---|---|---|---|---|
| Poor | 15.3 | 21.7 | 19.5 | 21.3 | 34.2 |
| Low Income | 16.7 | 20.7 | 25.0 | 28.6 | 40.3 |
| Middle Income | 23.9 | 30.3 | 30.3 | 40.2 | 47.8 |
| High Income | 32.6 | 43.2 | 41.6 | 46.8 | 64.3 |
Source: Centers for Disease Control and Prevention, National Center for Health Statistics, National Health Interview Survey, 2000-2010.
Denominator: Adults ages 50-75.
Note: Measure is age adjusted.
- Importance: Screening can detect abnormal colorectal growths before they develop into cancer. Early detection increases treatment options and the chances for cure. Effective screening modalities include fecal occult blood testing (FOBT), FOBT with flexible sigmoidoscopy, and colonoscopy.
- Trends: From 2000 to 2010, the percentage of adults ages 50-75 who received appropriate colorectal cancer screening increased overall and among all racial/ethnic groups.
- Groups With Disparities:
- In all years, the percentage of adults who received appropriate colorectal cancer screening was lower among Hispanics and Blacks compared with Whites.
- In all years, the percentage of adults who received appropriate colorectal cancer screening was lower among poor and low-income Hispanics compared with high-income Hispanics.
Slide 28
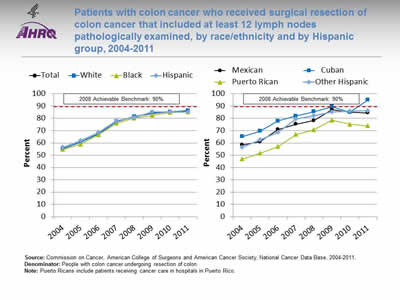
Patients with colon cancer who received surgical resection of colon cancer that included at least 12 lymph nodes pathologically examined, by race/ethnicity and by Hispanic group, 2004-2011
Image: Graphs show patients with colon cancer who received surgical resection of colon cancer that included at least 12 lymph nodes pathologically examined:
Left Graph:
| Race/Ethnicity | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 |
|---|---|---|---|---|---|---|---|---|
| Total | 55.4 | 60.5 | 67.4 | 77.4 | 81.4 | 84.2 | 85.3 | 86.2 |
| White | 55.3 | 60.7 | 67.3 | 77.4 | 81.6 | 84.5 | 85.4 | 86.4 |
| Black | 54.6 | 58.9 | 66.6 | 76.1 | 80.2 | 82.4 | 84.9 | 85.2 |
| Hispanic | 56.3 | 61.8 | 68.7 | 78.0 | 81.0 | 85.1 | 85.1 | 85.2 |
2008 Achievable Benchmark: 90%.
Right Graph:
| Hispanic Group | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 |
|---|---|---|---|---|---|---|---|---|
| Mexican | 58.4 | 60.9 | 71.0 | 75.2 | 78.2 | 87.2 | 84.9 | 84.5 |
| Cuban | 65.1 | 69.6 | 77.8 | 81.9 | 85.5 | 89.5 | 84.9 | 94.9 |
| Puerto Rican | 46.9 | 51.6 | 57.0 | 66.9 | 70.8 | 78.5 | 75.2 | 73.9 |
| Other Hispanic | 56.5 | 62.6 | 68.6 | 79.3 | 82.0 | 85.2 | 86.0 | 86.1 |
2008 Achievable Benchmark: 90%.
Source: Commission on Cancer, American College of Surgeons and American Cancer Society, National Cancer Data Base, 2004-2011.
Denominator: People with colon cancer undergoing resection of colon.
Note: Puerto Ricans include patients receiving cancer care in hospitals in Puerto Rico.
- Importance: Recommended cancer treatment depends on different factors, such as the stage or extent of the cancer within the body, especially whether the disease has spread from the original site to other parts of the body. Colon cancer typically begins as a benign polyp that may become cancerous and then spread to local lymph nodes. Hence, ensuring adequate examination of lymph nodes when surgery is performed is important.
- Trends: From 2004 to 2011, the percentage of patients with colon cancer who received surgical resection of colon cancer that included at least 12 lymph nodes pathologically examined improved overall and for all racial/ethnic groups.
- Groups With Disparities:
- In all but 1 year, Puerto Ricans were less likely than Whites to have surgical resection of colon cancer that included at least 12 lymph nodes examined.
- Achievable Benchmark:
- The 2008 top 5 State achievable benchmark was 90%. The top 5 States that contributed to the achievable benchmark are Delaware, Missouri, Utah, Vermont, and Wisconsin.
- At the current rates of improvement, the achievable benchmark could be attained overall and for all racial/ethnic groups within a year.
- Cubans have already achieved the benchmark while Puerto Ricans would not reach the benchmark for 4 years.
Slide 29
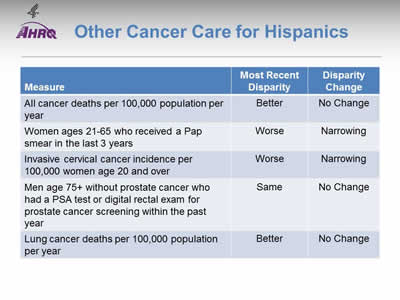
Other Cancer Care for Hispanics
| Measure | Most Recent Disparity | Disparity Change |
|---|---|---|
| All cancer deaths per 100,000 population per year | Better | No Change |
| Women ages 21-65 who received a Pap smear in the last 3 years | Worse | Narrowing |
| Invasive cervical cancer incidence per 100,000 women age 20 and over | Worse | Narrowing |
| Men age 75+ without prostate cancer who had a PSA test or digital rectal exam for prostate cancer screening within the past year | Same | No Change |
| Lung cancer deaths per 100,000 population per year | Better | No Change |
Note:
- Trends: Most measures of other cancer care for Hispanics were improving.
- Groups With Disparities:
- Death rates were lower among Hispanics compared with Whites and were not changing over time for:
- All cancers in aggregate.
- Lung cancer.
- Death rates were lower among Hispanics compared with Whites and were not changing over time for:
- Hispanics were less likely to receive appropriate Pap testing and more likely to develop invasive cervical cancer compared with Whites. These disparities were narrowing over time.
Slide 30

Women ages 21-65 who received a Pap smear in the last 3 years, by race/ethnicity and by insurance among Hispanics, 2000-2010
Image: Graphs show women ages 21-65 who received a Pap smear in the last 3 years:
Left Graph:
| Race/Ethnicity | 2000 | 2005 | 2008 | 2010 |
|---|---|---|---|---|
| Total | 87.5 | 85.3 | 84.5 | 82.8 |
| Hispanic | 80.9 | 79.3 | 81.3 | 78.5 |
| Black | 90.4 | 84.9 | 86.1 | 84.6 |
| White | 89.1 | 87.5 | 86.1 | 84.5 |
Right Graph (Hispanics):
| Insurance | 2000 | 2005 | 2008 | 2010 |
|---|---|---|---|---|
| Private | 88.0 | 87.9 | 87.8 | 86.6 |
| Public | 87.0 | 77.4 | 87.4 | 84.8 |
| Uninsured | 69.6 | 69.3 | 70.1 | 65.3 |
Source: Centers for Disease Control and Prevention, National Center for Health Statistics, National Health Interview Survey, 2000-2010.
Denominator: Women ages 21-65.
Note: Measure is age adjusted.
- Importance: Screening with Pap smears can detect high-grade precancerous cervical lesions that can be removed before they become cancerous.
- Trends: From 2000 to 2010, the percentage of women ages 21-65 who received a Pap smear in the last 3 years decreased overall and among White women; no statistically significant changes were noted among Hispanic women.
- Groups With Disparities:
- In all years, the percentage of women who received a Pap smear was lower among Hispanic women compared with White women.
- In all years, the percentage of women who received a Pap smear was lower among uninsured Hispanic women compared with privately insured Hispanic women.
Slide 31
AHRQ Health Care Innovations in Cancer Screening
Family Health Partnership Clinic
- Location: McHenry County, Illinois.
- Population: Rural, low-income Hispanic women >40.
- Intervention: Celebremos La Vida seeks to enhance access to culturally competent cancer screening and educational information by providing a monthly women's clinic.
- Outcomes: Enhanced access to breast and cervical cancer screening, increased use of primary care services, and high levels of patient satisfaction.
Slide 32

National Healthcare Quality and Disparities Report Chartbook on Health Care for Hispanics
Part 2: Trends in Priorities of the Heckler Report
Care for Cardivascular Diseases
Note:
- Thirty years ago, the Heckler Report found that:
- Cardiovascular disease (CVD) is a major cause of death in Hispanics, although the rate is lower than in Whites. To date, national epidemiologic data on CVD mortality in Hispanics are limited.
- There appears to be a strong inverse relationship between socioeconomic status (SES) and hypertension in Hispanics, similar to that found for Blacks and Whites.
- Diabetes mellitus is a major problem in Hispanics, especially in Mexican Americans and Puerto Ricans living in the United States.
- The generally higher prevalence of obesity, noninsulin-dependent diabetes, hypertension, high LDL cholesterol and low HDL cholesterol levels in Hispanics might be expected to increase their CVD risk. Those Mexican Americans with lowest SES and level of acculturation have significantly worse CVD risk factor profiles than those in higher SES groups.
Slide 33
Cardiovascular Care for Hispanics
| Measure | Most Recent Disparity | Disparity Change |
|---|---|---|
| Adults who received a blood pressure measurement in the last 2 years and can state whether their blood pressure was normal or high | Worse | No Change |
| Adult admissions for hypertension | Worse | No Change |
| Adult admissions for angina without cardiac procedure | Worse | No Change |
| Adult admissions for congestive heart failure | Same | Narrowing |
| Hospital patients with heart failure and left ventricular systolic dysfunction who were prescribed angiotensin-converting enzyme inhibitor or angiotensin receptor blocker at discharge | Better | No Change |
| Hospital patients with heart attack given percutaneous coronary intervention within 90 minutes of arrival | Worse | No Change |
| Hospital patients with heart attack given fibrinolytic medication within 30 minutes of arrival | Same | No Change |
Note:
- Trends: Most measures of cardiovascular care for Hispanics were improving.
- Groups With Disparities:
- Hispanics were less likely than Whites to have their blood pressure checked and to receive timely percutaneous coronary intervention when hospitalized with a heart attack. These disparities did not change over time.
- Hispanics had higher rates of admission than Whites for hypertension and for angina and these disparities did not change over time.
- Hispanics and Whites had similar rates of admission for congestive heart failure. This represents the elimination of a previously observed disparity.
- Hispanics and Whites had similar rates of receipt of fibrinolytic medication for heart attack.
- Hispanics hospitalized with heart failure were more likely to be prescribed angiotensin-converting enzyme inhibitor or angiotensin receptor blocker at discharge and this disparity did not change over time.
Slide 34
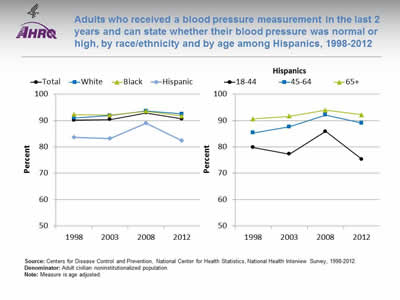
Adults who received a blood pressure measurement in the last 2 years and can state whether their blood pressure was normal or high, by race/ethnicity and by age among Hispanics, 1998-2012
Image: Graphs show adults who received a blood pressure measurement in the last 2 years and can state whether their blood pressure was normal or high:
Left Graph:
| Race/Ethnicity | 1998 | 2003 | 2008 | 2012 |
|---|---|---|---|---|
| Total | 90.1 | 90.4 | 92.9 | 90.6 |
| White | 91.0 | 91.9 | 93.6 | 92.5 |
| Black | 92.3 | 92.1 | 93.5 | 91.7 |
| Hispanic | 83.6 | 83.2 | 89.0 | 82.4 |
Right Graph (Hispanics):
| Age | 1998 | 2003 | 2008 | 2012 |
|---|---|---|---|---|
| 18-44 | 79.8 | 77.3 | 85.9 | 75.3 |
| 45-64 | 85.3 | 87.6 | 92.1 | 89.0 |
| 65+ | 90.6 | 91.6 | 93.9 | 92.2 |
Source: Centers for Disease Control and Prevention, National Center for Health Statistics, National Health Interview Survey, 1998-2012.
Denominator: Adult civilian noninstitutionalized population.
Note: Measure is age adjusted.
- Importance: Early detection and treatment of high blood pressure can prevent heart failure, kidney failure, and stroke. Because high blood pressure typically causes no symptoms, screening is essential.
- Trends: From 1998 to 2012, the percentage of adults who received a blood pressure measurement in the last 2 years and can state whether their blood pressure was normal or high did not change overall or for any racial/ethnic group.
- Groups With Disparities:
- In all years, Hispanic adults were less likely to receive a blood pressure measurement compared with Whites.
- In all years, Hispanics ages 18-44 were less likely to receive a blood pressure measurement compared with Hispanics age 65 and over.
Slide 35
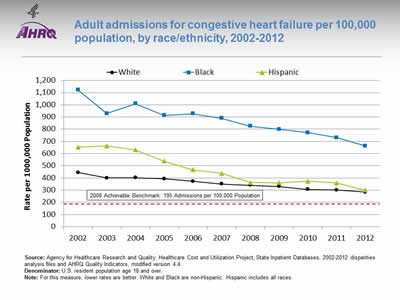
Adult admissions for congestive heart failure per 100,000 population, by race/ethnicity, 2002-2012
Image: Graph shows adult admissions for congestive heart failure per 100,000 population:
| Year | White | Black | Hispanic |
|---|---|---|---|
| 2002 | 444.1 | 1121.8 | 653.0 |
| 2003 | 399.5 | 927.8 | 662.2 |
| 2004 | 400.9 | 1009.3 | 629.9 |
| 2005 | 392.8 | 912.4 | 538.0 |
| 2006 | 373.0 | 927.5 | 465.9 |
| 2007 | 350.8 | 890.2 | 437.1 |
| 2008 | 339.9 | 824.6 | 362.8 |
| 2009 | 329.7 | 799.2 | 360.2 |
| 2010 | 306.3 | 771.4 | 372.7 |
| 2011 | 301.1 | 730.5 | 359.2 |
| 2012 | 283.2 | 662.2 | 298.9 |
2008 Achievable Benchmark: 195 Admissions per 100,000 Population.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases, 2002-2012 disparities analysis files and AHRQ Quality Indicators, modified version 4.4.
Denominator: U.S. resident population age 18 and over.
Note: For this measure, lower rates are better. White and Black are non-Hispanic. Hispanic includes all races.
- Importance: Racial disparities in care for congestive heart failure have been observed.
- Trends: From 2002 to 2012, the rate of admission for congestive heart failure among adults decreased significantly for all racial/ethnic groups.
- Groups With Disparities:
- In all years, compared with White patients, rates of admission for congestive heart failure were higher among Black patients.
- From 2002 to 2007, rates of admission for congestive heart failure were higher among Hispanic patients compared with White patients; in more recent years, this disparity was eliminated.
- Achievable Benchmark:
- The 2008 top 4 State achievable benchmark for adult congestive heart failure admissions was 195 admissions per 100,000 population. The top 4 States that contributed to the achievable benchmark are Colorado, Oregon, Utah, and Vermont.
- At current rates of improvement, Hispanic patients could achieve the benchmark in 3 years and White patients could achieve it in 6 years. Black patients would need 12 years to achieve the benchmark.
Slide 36
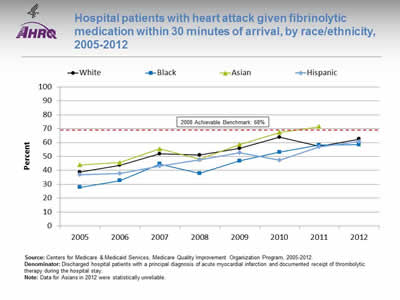
Hospital patients with heart attack given fibrinolytic medication within 30 minutes of arrival, by race/ethnicity, 2005-2012
Image: Graph shows hospital patients with heart attack given fibrinolytic medication within 30 minutes of arrival:
| Race/Ethnicity | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 |
|---|---|---|---|---|---|---|---|---|
| White | 38.7 | 43.6 | 51.8 | 51.0 | 55.7 | 63.8 | 57.3 | 62.5 |
| Black | 27.7 | 32.6 | 44.5 | 37.8 | 46.8 | 53 | 58.2 | 58.5 |
| Hispanic | 36.8 | 37.8 | 43.2 | 47.6 | 52.8 | 47.3 | 57 | 60.8 |
| Asian | 43.9 | 45.5 | 55.5 | 48.2 | 58.6 | 67.3 | 71.4 |
2008 Achievable Benchmark: 68%.
Source: Centers for Medicare & Medicaid Services, Medicare Quality Improvement Organization Program, 2005-2012.
Denominator: Discharged hospital patients with a principal diagnosis of acute myocardial infarction and documented receipt of thrombolytic therapy during the hospital stay.
Note: Data for Asians in 2012 were statistically unreliable.
- Importance: Some heart attacks are caused by blood clots. Early actions, such as fibrinolytic medication, may open blockages caused by blood clots, reduce heart muscle damage, and save lives. To be effective, these actions need to be performed quickly after the start of a heart attack.
- Trends: From 2005 to 2012, the percentage of patients who received timely fibrinolytic medication improved overall and for all racial/ethnic groups.
- Groups With Disparities: Until 2011, the percentage of patients who received timely fibrinolytic medication was significantly higher for Whites than for Blacks.
- Achievable Benchmark:
- The 2010 top 5 State achievable benchmark was 68%. The top 5 States that contributed to the achievable benchmark are Arkansas, California, Georgia, Mississippi, and Texas.
- Asian heart attack patients achieved the benchmark in 2011.
- At the current rate of improvement, the achievable benchmark could be attained overall in 2 years. In addition, White, Black, and Hispanic heart attack patients should all reach the benchmark in 2 years.
Slide 37
Outcomes of Cardiovascular Care for Hispanics
| Measure | Most Recent Disparity | Disparity Change |
|---|---|---|
| Deaths per 1,000 hospital admissions with acute myocardial infarction (AMI), age 18+ | Same | No Change |
| Deaths per 1,000 hospital admissions with congestive heart failure (CHF), age 18+ | Better | No Change |
| Deaths per 1,000 hospital admissions with abdominal aortic aneurysm repair, age 18+ | Same | No Change |
| Deaths per 1,000 hospital admissions with coronary artery bypass graft, age 40+ | Same | No Change |
| Deaths per 1,000 hospital admissions with percutaneous transluminal coronary angioplasty, age 40+ | Same | No Change |
Note:
- Trends: Most measures of deaths from cardiovascular care for Hispanics were improving.
- Groups With Disparities:
- Hispanics and Whites had similar death rates when hospitalized for:
- Acute myocardial infarction.
- Abdominal aortic aneurysm repair.
- Coronary artery bypass graft surgery.
- Percutaneous transluminal coronary angioplasty.
- Hispanics and Whites had similar death rates when hospitalized for:
- Hispanics had lower death rates than Whites when hospitalized for congestive heart failure and there was no change in this disparity over time.
Slide 38
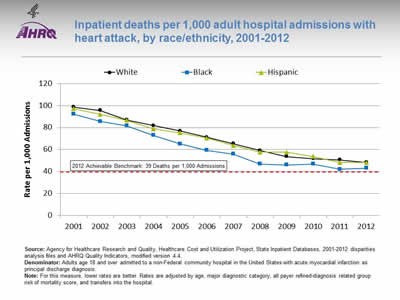
Inpatient deaths per 1,000 adult hospital admissions with heart attack, by race/ethnicity, 2001-2012
Image: Graph shows inpatient deaths per 1,000 adult hospital admissions with heart attack:
| Year | White | Black | Hispanic |
|---|---|---|---|
| 2001 | 98.7 | 92.2 | 97.2 |
| 2002 | 95.5 | 85.5 | 92.0 |
| 2003 | 86.9 | 81.6 | 86.6 |
| 2004 | 81.8 | 72.9 | 78.8 |
| 2005 | 76.9 | 65.2 | 75.2 |
| 2006 | 71.2 | 59.2 | 70.4 |
| 2007 | 65.4 | 55.8 | 63.6 |
| 2008 | 59.1 | 46.8 | 57.6 |
| 2009 | 53.7 | 46.1 | 57.5 |
| 2010 | 51.7 | 46.7 | 53.6 |
| 2011 | 50.5 | 42.1 | 48.1 |
| 2012 | 48.3 | 43.0 | 48.0 |
2012 Achievable Benchmark: 39 Deaths per 1,000 Admissions.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases, 2001‐2012 disparities analysis files and AHRQ Quality Indicators, modified version 4.4.
Denominator: Adults age 18 and over admitted to a non-Federal community hospital in the United States with acute myocardial infarction as principal discharge diagnosis.
Note: For this measure, lower rates are better. Rates are adjusted by age, major diagnostic category, all payer refined-diagnosis related group risk of mortality score, and transfers into the hospital.
- Importance: Racial disparities in heart attack care have been observed.
- Trends: From 2001 to 2012, the risk-adjusted inpatient mortality rate for hospital admissions with heart attack decreased significantly for all racial/ethnic groups.
- Groups With Disparities: In 2012, Black patients had lower inpatient mortality rates for hospital admissions with heart attack than White patients.
- Achievable Benchmark:
- The 2008 top 4 State achievable benchmark for inpatient heart attack mortality was 48 deaths per 1,000 admissions. By 2012, this benchmark had been attained for all racial/ethnic groups.
- Because the 2008 benchmark was achieved by the total population, a new 2012 top 4 State achievable benchmark was set at 39 deaths per 1,000 admissions. The top 4 States that contributed to the achievable benchmark are Alaska, Arizona, Michigan, and Rhode Island.
- At current rates of improvement, all racial/ethnic groups could reach the 2012 benchmark in approximately 2 years.
Slide 39

National Healthcare Quality and Disparities Report Chartbook on Health Care for Hispanics
Part 2: Trends in Priorities of the Heckler Report
Care for Substance Use Disorders
Note:
- Thirty years ago, the Heckler Report found that:
- Mortality statistics for the United States do not identify Hispanics separately, and until 1976, most other common measures of alcohol-related problems such as arrest and hospital discharge rates did not provide a Hispanic identifier. The 1979 National Institute on Alcohol Abuse and Alcoholism National Survey indicates that based on self-reported data, Hispanic American males age 18 and over have higher levels of heavy drinking and higher rates of alcohol-related problems than do nonminorities.
- Results from the 1983 single-room occupancy hotels study of drug abuse in New York City suggest that Hispanics have higher rates of drug use than Whites for marijuana, cocaine, heroin, and illicit methadone.
- Lung and esophageal cancer morbidity and mortality rates, known to be related to smoking, are lower for Hispanics than for Whites and Blacks.
Slide 40
Care for Substance Use Disorders for Hispanics
| Measure | Most Recent Disparity | Disparity Change |
|---|---|---|
| People age 12 and over who received any illicit drug or alcohol abuse treatment in the last 12 months | Same | No Change |
| People age 12 and over who needed treatment for illicit drug use or an alcohol problem and who received such treatment at a specialty facility in the last 12 months | Same | No Change |
| People age 12 and over treated for substance abuse who completed treatment course | Same | No Change |
Note:
- Trends: No measure of care for substance use disorders was improving for Hispanics.
- Groups With Disparities: Hispanics and Whites had similarly low rates of treatment for substance use disorders.
Slide 41
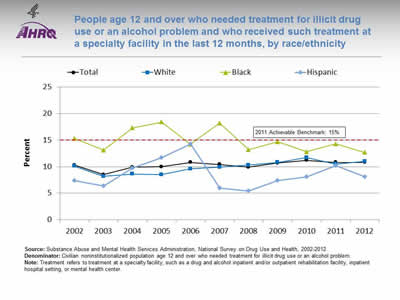
People age 12 and over who needed treatment for illicit drug use or an alcohol problem and who received such treatment at a specialty facility in the last 12 months, by race/ethnicity
Image: Graph shows people age 12 and over who needed treatment for illicit drug use or an alcohol problem and who received such treatment at a specialty facility in the last 12 months:
| Race/Ethnicity | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | 10.3 | 8.5 | 9.9 | 10.0 | 10.8 | 10.4 | 9.9 | 10.7 | 11.2 | 10.8 | 10.8 |
| White | 10.1 | 8.2 | 8.6 | 8.5 | 9.6 | 9.9 | 10.3 | 10.8 | 11.7 | 10.5 | 11.0 |
| Black | 15.3 | 13.1 | 17.3 | 18.4 | 14.2 | 18.2 | 13.2 | 14.7 | 12.8 | 14.3 | 12.7 |
| Hispanic | 7.4 | 6.4 | 9.7 | 11.7 | 14.3 | 6.0 | 5.4 | 7.4 | 8.1 | 10.2 | 8.1 |
2011 Achievable Benchmark: 15%.
Source: Substance Abuse and Mental Health Services Administration, National Survey on Drug Use and Health, 2002-2012.
Denominator: Civilian noninstitutionalized population age 12 and over who needed treatment for illicit drug use or an alcohol problem.
Note: Treatment refers to treatment at a specialty facility, such as a drug and alcohol inpatient and/or outpatient rehabilitation facility, inpatient hospital setting, or mental health center.
- Overall Rate: In 2012, only 10.8% of people age 12 and over who needed treatment for illicit drug use or an alcohol problem received such treatment at a specialty facility in the last 12 months.
- Groups With Disparities: From 2002 to 2012, there were no statistically significant differences by race/ethnicity.
- Achievable Benchmark:
- The 2011 top 6 State achievable benchmark was 15%. The top 6 States that contributed to the achievable benchmark are Alabama, Alaska, Delaware, Maryland, Oregon, and Utah.
- At the current rate, the total population would need 30 years to achieve this benchmark. Whites could achieve the benchmark in 15 years while Blacks and Hispanics are moving away from the benchmark.
Slide 42
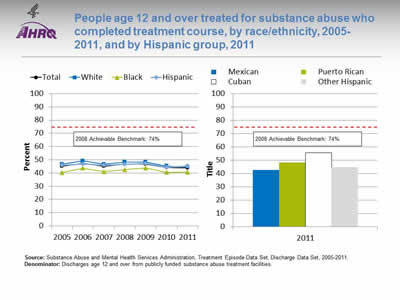
People age 12 and over treated for substance abuse who completed treatment course, by race/ethnicity, 2005-2011, and by Hispanic group, 2011
Image: Graph and bar chart show people age 12 and over treated for substance abuse who completed treatment course:
Left Graph:
| Race/Ethnicity | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 |
|---|---|---|---|---|---|---|---|
| Total | 45.0 | 47.5 | 45.1 | 46.6 | 46.7 | 44.1 | 43.7 |
| Hispanic | 46.0 | 46.7 | 45.8 | 46.5 | 47.1 | 44.4 | 45.3 |
| White | 46.7 | 49.2 | 46.6 | 48.3 | 48.3 | 45.3 | 44.5 |
| Black | 40.4 | 43.6 | 41.0 | 42.5 | 43.8 | 40.6 | 40.7 |
2008 Achievable Benchmark: 74%.
Right Graph (Hispanic Group):
- Mexican - 42.8.
- Puerto Rican - 48.3.
- Cuban - 55.7.
- Other Hispanic - 44.8.
2008 Achievable Benchmark: 74%.
Source: Substance Abuse and Mental Health Services Administration, Treatment Episode Data Set, Discharge Data Set, 2005-2011.
Denominator: Discharges age 12 and over from publicly funded substance abuse treatment facilities.
Note:
- Overall Rate: In 2011, 43.7% of people age 12 and over treated for substance abuse completed their treatment course.
- Groups With Disparities:
- In 4 of 7 years, Blacks who were treated for substance abuse were significantly less likely than Whites to complete treatment.
- Hispanics and Whites had similar rates of treatment completion.
- In 2011, Cubans who were treated for substance abuse were significantly more likely than Whites to complete treatment.
- Achievable Benchmark:
- The 2008 top 5 State achievable benchmark was 74%. The top 5 States that contributed to the achievable benchmark are Colorado, Connecticut, District of Columbia, Mississippi, and Texas.
- No group showed progress toward the benchmark.
Slide 43

National Healthcare Quality and Disparities Report Chartbook on Health Care for Hispanics
Part 2: Trends in Priorities of the Heckler Report
Care for Diabetes
Note:
- Thirty years ago, the Heckler Report found that:
- Among the 14.6 million individuals of Hispanic origin in the United States, the prevalence of diabetes was more than three times the rate in the White population.
- From available data, it is clear than diabetes is a major health burden contributing to excess morbidity and mortality in the Mexican American population. The data are still inadequate, however, to say with certainty whether this increased prevalence of diabetes is shared by other Hispanic subgroups.
Slide 44
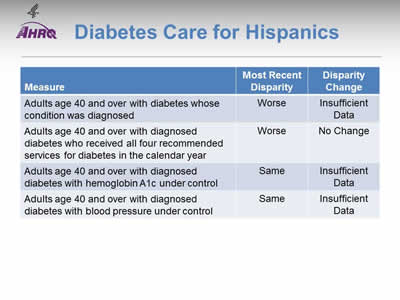
Diabetes Care for Hispanics
| Measure | Most Recent Disparity | Disparity Change |
|---|---|---|
| Adults age 40 and over with diabetes whose condition was diagonsed | Worse | Insufficient Data |
| Adults age 40 and over with diagnosed diabetes who received all four recommended services for diabetes in the calendar year | Worse | No Change |
| Adults age 40 and over with diagnosed diabetes with hemoglobin A1c under control | Same | Insufficient Date |
| Adults age 40 and over with diagnosed diabetes with blood pressure under control | Same | Insufficient Data |
Note:
- Trends: Data are insufficient to assess trends for most measures of diabetes care for Hispanics.
- Groups With Disparities:
- Hispanics were less likely than Whites to have their diabetes diagnosed.
- After diagnosis, Hispanics were less likely than Whites to receive recommended services for diabetes and this disparity was not changing over time.
Slide 45
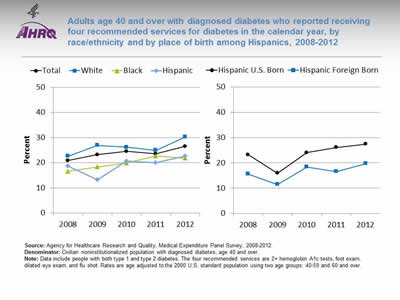
Adults age 40 and over with diagnosed diabetes who reported receiving four recommended services for diabetes in the calendar year, by race/ethnicity and by place of birth among Hispanics, 2008-2012
Image: Graphs show adults age 40 and over with diagnosed diabetes who reported receiving four recommended services for diabetes in the calendar year:
Left Graph:
| Race/Ethnicity | 2008 | 2009 | 2010 | 2011 | 2012 |
|---|---|---|---|---|---|
| Total | 21.0 | 23.2 | 24.6 | 23.6 | 26.6 |
| White | 22.7 | 26.9 | 26.2 | 25.0 | 30.3 |
| Black | 16.6 | 18.3 | 20.0 | 22.8 | 21.8 |
| Hispanic | 18.7 | 13.3 | 20.7 | 20.1 | 22.7 |
Right Graph:
| Place of Birth | 2008 | 2009 | 2010 | 2011 | 2012 |
|---|---|---|---|---|---|
| Hispanic U.S. Born | 23.3 | 15.9 | 24.1 | 26.1 | 27.5 |
| Hispanic Foreign Born | 15.6 | 11.4 | 18.4 | 16.6 | 19.7 |
Source: Agency for Healthcare Research and Quality, Medical Expenditure Panel Survey, 2008-2012.
Denominator: Civilian noninstitutionalized population with diagnosed diabetes, age 40 and over.
Note: Data include people with both type 1 and type 2 diabetes. The four recommended services are 2+ hemoglobin A1c tests, foot exam, dilated eye exam, and flu shot. Rates are age adjusted to the 2000 U.S. standard population using two age groups: 40-59 and 60 and over.
- Importance:
- Regular hemoglobin A1c (HbA1c) tests, foot exams, dilated eye exams, and flu shots help people keep their diabetes under control and avoid diabetic complications.
- A composite measure is used to track the national rate of receipt of all four of these recommended annual diabetes interventions.
- Trends:
- From 2008 to 2012, among adults age 40 and over with diagnosed diabetes, improvements were observed overall and among Blacks.
- However, only slightly more than one-fourth (26.6 percent) of adults with diabetes reported receiving all four recommended services in 2012.
- Groups With Disparities:
- In 2 of 5 years, including 2012, Hispanics and Blacks were less likely than Whites to receive the recommended services.
- In all years, foreign-born Hispanics were less likely than U.S.-born Hispanics to receive the recommended services, but these differences were not statistically significant.
Slide 46
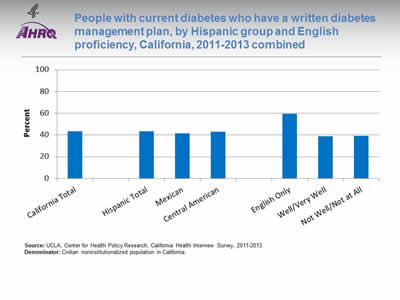
People with current diabetes who have a written diabetes management plan, by Hispanic group and English proficiency, California, 2011-2013 combined
Image: Chart shows people with current diabetes who have a written diabetes management plan. By Hispanic group: California Total - 43.2%; Hispanic Total - 43.3%; Mexican - 41.6%; Central American - 42.9%. By English proficiency: English Only - 59.4%; Well/Very Well - 38.9%; Not Well/Not at All - 39%.
Source: UCLA, Center for Health Policy Research, California Health Interview Survey, 2011-2013.
Denominator: Civilian noninstitutionalized population in California.
Note:
- Importance:
- A successful partnership for diabetes care requires providers to educate patients about daily management of their diabetes. Hence, providers should develop a written diabetes management plan, especially for patients with a history of uncontrolled diabetes.
- National data on diabetes management and outcomes for some underserved populations are not available from the national data sources in the QDR. These populations include people with limited English proficiency; individuals who speak a language other than English at home; and Hispanic subpopulations. To address some of these data gaps, we show additional data from the California Health Interview Survey.
- Overall Rate: Only 43% of Californians with current diabetes had a written diabetes management plan in 2011-2013.
- Groups With Disparities: Among Hispanic Californians with diabetes, those who spoke English well/very well and not well/not at all were less likely than those who spoke English only to have a written diabetes management plan.
Slide 47
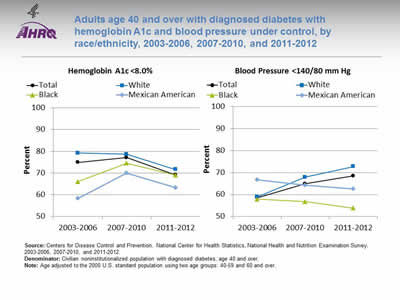
Adults age 40 and over with diagnosed diabetes with hemoglobin A1c and blood pressure under control, by race/ethnicity, 2003-2006, 2007-2010, and 2011-2012
Image: Graphs shows adults age 40 and over with diagnosed diabetes with hemoglobin A1c and blood pressure under control:
Left Graph (Hemoglobin A1c <8.0%):
| Race/Ethnicity | 2003-2006 | 2007-2010 | 2011-2012 |
|---|---|---|---|
| Total | 74.9 | 77.1 | 69.2 |
| Mexican American | 58.3 | 69.9 | 63.3 |
| Black | 66.0 | 74.5 | 69.1 |
| White | 79.2 | 78.6 | 71.6 |
Right Graph (Blood Pressure <140/80 mm Hg):
| Race/Ethnicity | 2003-2006 | 2007-2010 | 2011-2012 |
|---|---|---|---|
| Total | 58.5 | 64.9 | 68.5 |
| Mexican American | 66.8 | 64.2 | 62.5 |
| Black | 57.9 | 56.7 | 53.8 |
| White | 58.9 | 67.9 | 72.8 |
Source: Centers for Disease Control and Prevention, National Center for Health Statistics, National Health and Nutrition Examination Survey, 2003-2006, 2007-2010, and 2011-2012.
Denominator: Civilian noninstitutionalized population with diagnosed diabetes, age 40 and over.
Note: Age adjusted to the 2000 U.S. standard population using two age groups: 40-59 and 60 and over.
- Importance: People diagnosed with diabetes are often at higher risk for other cardiovascular risk factors, such as high blood pressure. Having these conditions in combination with diagnosed diabetes increases the likelihood of complications, such as heart and kidney diseases, blindness, nerve damage, and stroke. Patients who manage their diagnosed diabetes and maintain an HbA1c level <8% and blood pressure <140/80 mm Hg can decrease these risks.
- Overall Rate: Among adults age 40 and over with diagnosed diabetes, 69.2% achieved HbA1c less than 8% and 68.5% achieved blood pressure less than 140/80 mm Hg in 2011-2012.
- Groups With Disparities:
- In 2003-2006, Blacks and Mexican Americans were less likely than Whites to have their HbA1c under control. Differences in 2007-2010 and 2011-2012 were not statistically significant.
- In 2007-2010 and 2011-2012, Blacks were less likely than Whites to have their blood pressure under control.
Slide 48
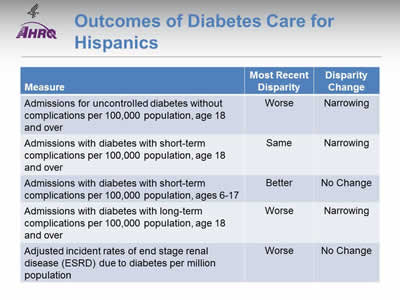
Outcomes of Diabetes Care for Hispanics
- Trends: Most outcomes of diabetes care for Hispanics were improving.
- Groups with Disparities:
- Hispanics had higher rates of admission than Whites for uncontrolled diabetes and for long-term complications of diabetes. These disparities were narrowing over time.
- Hispanic adults and White adults had similar rates of admission for short-term complications of diabetes. This represents the elimination of a previously observed disparity.
- Hispanic children had lower rates of admission than White children and this disparity was not changing over time.
- Hispanics had higher rates of ESRD due to diabetes than Whites and this disparity was not changing over time.
Slide 49
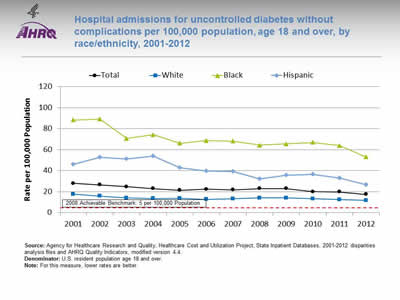
Hospital admissions for uncontrolled diabetes without complications per 100,000 population, age 18 and over, by race/ethnicity, 2001-2012
Image: Graph shows hospital admissions for uncontrolled diabetes without complications per 100,000 population:
| Race/Ethnicity | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | 27.9 | 26.4 | 24.8 | 23.0 | 21.2 | 22.4 | 21.8 | 23.0 | 22.9 | 20.0 | 19.8 | 17.3 |
| White | 17.6 | 15.8 | 14.0 | 13.5 | 13.6 | 12.6 | 13.2 | 14.1 | 14.0 | 13.1 | 12.4 | 11.7 |
| Black | 88.3 | 89.1 | 70.6 | 74.2 | 66.1 | 68.7 | 68.1 | 64.4 | 65.5 | 66.9 | 64.0 | 53.1 |
| Hispanic | 46.0 | 52.9 | 51.1 | 53.8 | 42.9 | 39.8 | 39.3 | 32.2 | 35.8 | 36.4 | 33.1 | 26.7 |
2008 Achievable Benchmark: 5 per 100,000 Population.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases, 2001‐2012 disparities analysis files and AHRQ Quality Indicators, modified version 4.4.
Denominator: U.S. resident population age 18 and over.
Note: For this measure, lower rates are better.
- Importance:
- Individuals who do not achieve good control of their diabetes may develop symptoms that require correction through hospitalization.
- Admission rates for uncontrolled diabetes may be reduced by better outpatient treatment and patients' tighter adherence to the recommended diet and medication.
- Trends:
- The rate of hospital admissions for uncontrolled diabetes without complications per 100,000 population decreased from 27.9 in 2001 to 17.3 in 2012.
- From 2001 to 2012, the rate of hospital admissions per 100,000 population decreased for all populations:
- For Hispanics, from 46.0 to 26.7.
- For Blacks, from 88.3 to 53.1.
- For Whites, from 17.6 to 11.7.
- Groups With Disparities: In all years, the rate of hospital admissions for uncontrolled diabetes was higher for Blacks and Hispanics compared with Whites.
- Achievable Benchmark:
- The 2008 top 4 State achievable benchmark was 5 admissions per 100,000 population age 18 and over. The top 4 States that contributed to the achievable benchmark are Colorado, Hawaii, Utah, and Vermont.
- At the current rate, the benchmark could not be met for the total population for approximately 17 years.
- At the current rates, Whites could not reach the benchmark for 22 years and Blacks would need 20 years. Hispanics could reach the benchmark in 10 years.
Slide 50
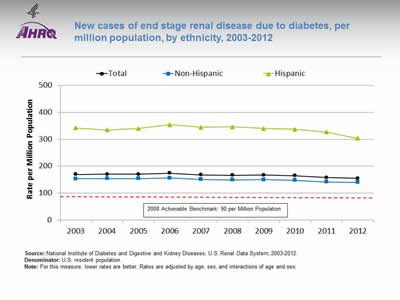
New cases of end stage renal disease due to diabetes, per million population, by ethnicity, 2003-2012
Image: Graph shows new cases of end stage renal disease due to diabetes, per million population:
| Ethnicity | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 |
|---|---|---|---|---|---|---|---|---|---|---|
| Total | 169.5 | 169.6 | 170.2 | 173.6 | 167.9 | 165.8 | 166.7 | 164.2 | 157.7 | 154.3 |
| Hispanic | 342.7 | 334.7 | 340.3 | 353.7 | 345.1 | 346.3 | 339.8 | 336.7 | 326.8 | 303.8 |
| Non-Hispanic | 152.6 | 153.6 | 153.9 | 156.4 | 150.9 | 148.7 | 150.2 | 147.7 | 141.4 | 140.0 |
2008 Achievable Benchmark: 90 per Million Population.
Source: National Institute of Diabetes and Digestive and Kidney Diseases, U.S. Renal Data System, 2003-2012.
Denominator: U.S. resident population.
Note: For this measure, lower rates are better. Rates are adjusted by age, sex, and interactions of age and sex.
- Importance: Diabetes is the most common cause of kidney failure. Keeping blood glucose levels under control can prevent or slow the progression of kidney disease. When kidney disease is detected early, medication can slow the disease's progress; when detected late, it commonly progresses to end stage renal disease requiring dialysis or kidney transplantation. While some cases of kidney failure due to diabetes cannot be avoided, other cases reflect inadequate control of blood glucose or delayed detection and treatment of early kidney disease due to diabetes.
- Trends: From 2003 to 2012, the overall rate of new cases of ESRD due to diabetes improved for Hispanics.
- Groups With Disparities: In all years, Hispanics had higher rates than non-Hispanics.
- Achievable Benchmark:
- The 2008 top 5 State achievable benchmark was 90 per million population. The top 5 States that contributed to the achievable benchmark are Alaska, Maine, New Hampshire, Rhode Island, and Vermont.
- At current rates of change, the benchmark would not be achieved overall or by any ethnic group for decades.
Slide 51
National Healthcare Quality and Disparities Report Chartbook on Health Care for Hispanics
Part 2: Trends in Priorities of the Heckler Report
Suicide Prevention and Mental Health Care
Note:
- Thirty years ago, the Heckler Report found that:
- National data are not available for homicide deaths among Hispanic populations, but data from the five-State southwestern region, where more than 60% of Hispanics reside, show that from 1976 to 1980, the homicide rate was 21.6 per 100,000, more than 2.5 times the rate of the White population (7.7 per 100,000) in the same geographic area.
Slide 52
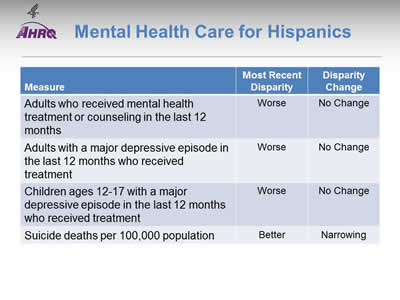
Mental Health Care for Hispanics
Note:
- Trends: No measure of mental health care for Hispanics was improving; suicide deaths were increasing.
- Groups With Disparities:
- Hispanic adults were less likely than White adults to receive mental health treatment or counseling and this disparity was not changing over time.
- When experiencing a major depressive episode, Hispanic adults and adolescents were less likely than Whites to receive treatment. These disparities were not changing over time.
- Hispanics had lower suicide death rates than Whites, but this disparity was narrowing as Hispanic suicide deaths increased.
Slide 53
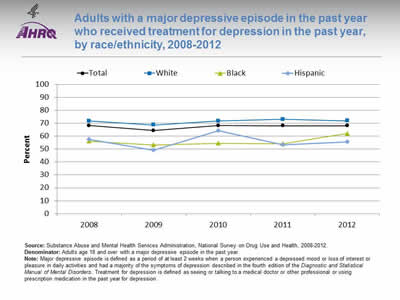
Adults with a major depressive episode in the past year who received treatment for depression in the past year, by race/ethnicity, 2008-2012
Image: Graph shows adults with a major depressive episode in the past year who received treatment for depression in the past year:
Source: Substance Abuse and Mental Health Services Administration, National Survey on Drug Use and Health, 2008-2012.
Denominator: Adults age 18 and over with a major depressive episode in the past year.
Note: Major depressive episode is defined as a period of at least 2 weeks when a person experienced a depressed mood or loss of interest or pleasure in daily activities and had a majority of the symptoms of depression described in the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders. Treatment for depression is defined as seeing or talking to a medical doctor or other professional or using prescription medication in the past year for depression.
| Race/Ethnicity | 2008 | 2009 | 2010 | 2011 | 2012 |
|---|---|---|---|---|---|
| Total | 68.3 | 64.4 | 68.2 | 68.1 | 68.0 |
| White | 71.8 | 68.7 | 71.8 | 73.1 | 72.0 |
| Black | 56.1 | 53.2 | 54.5 | 54.3 | 62.1 |
| Hispanic | 57.4 | 49.3 | 64.2 | 53.2 | 55.6 |
- Importance: The United States Preventive Services Task Force (USPSTF) recommends screening adults for depression when staff-assisted depression care supports are in place to ensure accurate diagnosis, effective treatment , and followup (USPSTF, 2015*).
- Overall Rate: In 2012, 68% of adults with a major depressive episode received treatment for depression.
- Groups With Disparities:
- In all years, Black adults with depression were less likely than White adults to receive treatment.
- In every year except 2010, Hispanic adults with depression were less likely than White adults to receive treatment.
* Depression in adults: screening. Released December 2009. Current as of July 2015. http://www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/depression-in-adults-screening?ds=1&s=depression.
Slide 54
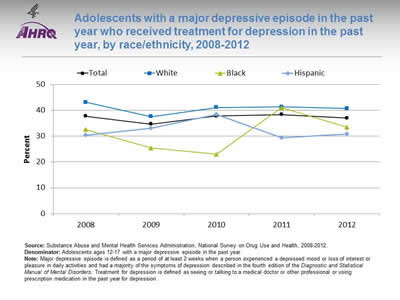
Adolescents with a major depressive episode in the past year who received treatment for depression in the past year, by race/ethnicity, 2008-2012
Image: Graph shows adolescents with a major depressive episode in the past year who received treatment for depression in the past year:
| Race/Ethnicity | 2008 | 2009 | 2010 | 2011 | 2012 |
|---|---|---|---|---|---|
| Total | 37.7 | 34.7 | 37.8 | 38.4 | 37.0 |
| White | 43.1 | 37.6 | 41.1 | 41.4 | 40.7 |
| Black | 32.6 | 25.4 | 23.0 | 41.0 | 33.5 |
| Hispanic | 30.3 | 33.1 | 38.4 | 29.4 | 30.8 |
Source: Substance Abuse and Mental Health Services Administration, National Survey on Drug Use and Health, 2008-2012.
Denominator: Adolescents ages 12-17 with a major depressive episode in the past year.
Note: Major depressive episode is defined as a period of at least 2 weeks when a person experienced a depressed mood or loss of interest or pleasure in daily activities and had a majority of the symptoms of depression described in the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders. Treatment for depression is defined as seeing or talking to a medical doctor or other professional or using prescription medication in the past year for depression.
- Importance:
- Outpatient mental health treatment and psychotropic medication use in children and adolescents increased in the United States between 1996-1998 and 2010-2012. Although youths with less severe or no impairment accounted for most of the absolute increase in service use, youths with more severe impairment had the greatest relative increase in use, yet less than half accessed services in 2010-2012 (Olfson, et al., 2015*).
- The United States Preventive Services Task Force (USPSTF) recommends screening of adolescents ages 12-18 years for major depressive disorder when systems are in place to ensure accurate diagnosis, psychotherapy (cognitive-behavioral or interpersonal), and followup (USPSTF, 2015**).
- Overall Rate: In 2012, 37% of adolescents with a major depressive episode received treatment for depression.
- Groups With Disparities: In 2012, Hispanic adolescents with depression were less likely than White adolescents to receive treatment.
* Olfson M1, Druss BG, Marcus SC. Trends in mental health care among children and adolescents. N Engl J Med 2015 May 21;372(21):2029-38.
** Depression in children and adolescents: screening. Released December 2009. Current as of July 2015. http://www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/depression-in-children-and-adolescents-screening?ds=1&s=depression.
Slide 55
AHRQ Health Care Innovations in Mental Health Care
University of Southern California
- Population: Low-income Hispanic patients with diabetes.
- Location: Los Angeles, California.
- Intervention: Worked with two safety net clinics to offer a socioculturally tailored program to treat depression.
- Outcomes: Improved long-term adherence to antidepressant medication, reduced depression-related symptoms, and increased patient satisfaction with depression care.
Slide 56
National Healthcare Quality and Disparities Report Chartbook on Health Care for Hispanics
Part 2: Trends in Priorities of the Heckler Report
Infant Mortality and Maternity Care
Note:
- Thirty years ago, the Heckler Report found that:
- There is considerable variation within the Hispanic population, and while postneonatal mortality rates are elevated, the birth weight distributions are generally favorable.
- Only 58% of Mexican American mothers begin prenatal care in the first trimester, less than for Blacks or Whites.
- The birth weight and hence infant mortality rates of U.S.-born Puerto Ricans are less favorable than those for Mexican Americans.
- Data on birth weight show a favorable distribution for Cubans.
Slide 57

Maternity Care for Hispanics
Note:
- Trends: Birth trauma and obstetric trauma were improving over time but other measures of maternity care were not changing.
- Groups With Disparities:
- Hispanics had lower rates of birth trauma and obstetric trauma than Whites and these disparities were not changing over time.
Slide 58
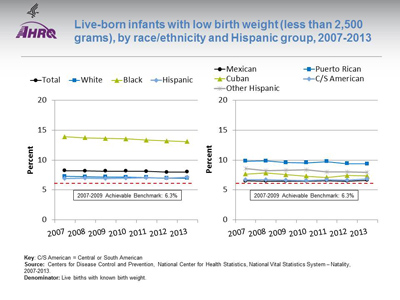
Live-born infants with low birth weight (less than 2,500 grams), by race/ethnicity and Hispanic group, 2007-2013
Image: Graphs show live-born infants with low birth weight:
Left Graph:
| Race/Ethnicity | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 |
|---|---|---|---|---|---|---|---|
| Total | 8.22 | 8.18 | 8.16 | 8.15 | 8.10 | 7.99 | 8.02 |
| White | 7.28 | 7.22 | 7.19 | 7.14 | 7.09 | 6.97 | 6.98 |
| Black | 13.90 | 13.71 | 13.61 | 13.53 | 13.33 | 13.18 | 13.08 |
| Hispanic | 6.93 | 6.96 | 6.94 | 6.97 | 7.02 | 6.97 | 7.09 |
2007-2009 Achievable Benchmark: 6.3%.
Right Graph:
| Hispanic Group | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 |
|---|---|---|---|---|---|---|---|
| Mexican | 6.50 | 6.49 | 6.47 | 6.49 | 6.55 | 6.48 | 6.62 |
| Puerto Rican | 9.83 | 9.86 | 9.59 | 9.55 | 9.75 | 9.40 | 9.38 |
| Cuban | 7.66 | 7.83 | 7.55 | 7.30 | 7.10 | 7.43 | 7.35 |
| C/S American | 6.71 | 6.70 | 6.64 | 6.55 | 6.70 | 6.64 | 6.85 |
| Other Hispanic | 8.61 | 8.24 | 8.28 | 8.38 | 8.02 | 8.00 | 7.99 |
2007-2009 Achievable Benchmark: 6.3%.
Key: C/S American = Central or South American
Source: Centers for Disease Control and Prevention, National Center for Health Statistics, National Vital Statistics System—Natality, 2007-2013.
Denominator: Live births with known birth weight.
Note:
- Importance: Low birth weight can put infants at risk of various complications and death. Adequate prenatal care can help ensure that babies are born full term and at a healthy weight.
- Trends: From 2007 to 2013, the percentage of live-born infants with low birth weight improved among Blacks but did not change overall or for Whites or Hispanics.
- Groups With Disparities:
- In all years, Black infants were more likely than White infants to be low birth weight.
- In all years, Puerto Rican infants were more likely than White infants to be low birth weight.
- Achievable Benchmark:
- The 2007-2009 top 5 State achievable benchmark was 6.3%. The top 5 States that contributed to the achievable benchmark are Alaska, Maine, Oregon, South Dakota, and Washington.
- Except Black infants, no groups showed movement toward the benchmark.
Slide 59

Live-born infants with very low birth weight (less than 1,500 grams), by race/ethnicity and Hispanic group, 2007-2013
Image: Graphs show live-born infants with very low birth weight:
Left Graph:
| Race/Ethnicity | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 |
|---|---|---|---|---|---|---|---|
| Total | 1.49 | 1.46 | 1.45 | 1.45 | 1.44 | 1.42 | 1.41 |
| White | 1.19 | 1.18 | 1.16 | 1.16 | 1.14 | 1.13 | 1.11 |
| Black | 3.20 | 3.01 | 3.06 | 2.98 | 2.99 | 2.94 | 2.9 |
| Hispanic | 1.21 | 1.20 | 1.19 | 1.20 | 1.20 | 1.22 | 1.21 |
Right Graph:
| Hispanic Group | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 |
|---|---|---|---|---|---|---|---|
| Mexican | 1.13 | 1.11 | 1.08 | 1.09 | 1.08 | 1.13 | 1.13 |
| Puerto Rican | 1.89 | 1.93 | 1.88 | 1.82 | 1.75 | 1.77 | 1.65 |
| Cuban | 1.27 | 1.43 | 1.46 | 1.42 | 1.30 | 1.55 | 1.27 |
| C/S American | 1.15 | 1.13 | 1.12 | 1.09 | 1.24 | 1.13 | 1.15 |
| Other Hispanic | 1.44 | 1.34 | 1.40 | 1.46 | 1.39 | 1.38 | 1.37 |
Key: C/S American = Central or South American
Source: Centers for Disease Control and Prevention, National Center for Health Statistics, National Vital Statistics System—Natality.
Denominator: Live births with known birth weight.
Note:
- Trends: From 2007 to 2013, the percentage of live-born infants with very low birth weight improved overall and among Whites and Blacks but did not change among Hispanics. This led to a widening of the Hispanic-White difference although it is still below our threshold for identifying statistically significant disparities.
- Groups With Disparities:
- In all years, Black infants were more likely than White infants to have very low birth weight.
- In all years, Puerto Rican infants were more likely than White infants to have very low birth weight.
Slide 60
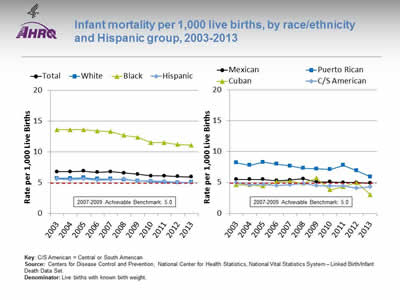
Infant mortality per 1,000 live births, by race/ethnicity and Hispanic group, 2003-2013
Image: Graphs show infant mortality per 1,000 live births:
Left Graph:
| Race/Ethnicity | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | 6.8 | 6.8 | 6.9 | 6.7 | 6.8 | 6.6 | 6.4 | 6.1 | 6.1 | 6.0 | 5.96 |
| White | 5.7 | 5.7 | 5.8 | 5.6 | 5.6 | 5.5 | 5.3 | 5.2 | 5.1 | 5.0 | 5.06 |
| Black | 13.6 | 13.6 | 13.6 | 13.4 | 13.3 | 12.7 | 12.4 | 11.5 | 11.5 | 11.2 | 11.11 |
| Hispanic | 5.6 | 5.5 | 5.6 | 5.4 | 5.5 | 5.6 | 5.3 | 5.3 | 5.2 | 5.1 | 5 |
2007-2009 Achievable Benchmark: 5.0.
Right Graph:
| Hispanic Group | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mexican | 5.5 | 5.5 | 5.5 | 5.3 | 5.4 | 5.6 | 5.1 | 5.1 | 5.0 | 5.0 | 4.9 |
| Puerto Rican | 8.2 | 7.8 | 8.3 | 8.0 | 7.7 | 7.3 | 7.2 | 7.1 | 7.8 | 6.9 | 5.93 |
| Cuban | 4.6 | 4.6 | 4.4 | 5.1 | 5.2 | 4.9 | 5.7 | 3.8 | 4.3 | 5.0 | 3.02 |
| C/S American | 5.0 | 4.6 | 4.7 | 4.5 | 4.6 | 4.8 | 4.5 | 4.4 | 4.4 | 4.1 | 4.3 |
2007-2009 Achievable Benchmark: 5.0.
Key: C/S American = Central or South American
Source: Centers for Disease Control and Prevention, National Center for Health Statistics, National Vital Statistics System—Linked Birth/Infant Death Data Set.
Denominator: Live births with known birth weight.
Note:
- Trends: From 2003 to 2013, the rate of infant mortality among live births improved overall and among Whites and Blacks but changes among Hispanics were not statistically significant.
- Groups With Disparities:
- In all years, mortality was higher among Black infants than White infants.
- In all years, mortality was higher among Puerto Rican infants than White infants.
- Achievable Benchmark:
- The 2007-2009 top 5 State achievable benchmark was 5 per 1,000 live births. The top 5 States that contributed to the achievable benchmark are California, Massachusetts, New Hampshire, Utah, and Washington.
- Hispanics, including Mexicans, Cubans, and Central and South Americans, have achieved the benchmark. Whites and Puerto Ricans are close to the benchmark. Blacks are farthest from the benchmark.
Slide 61
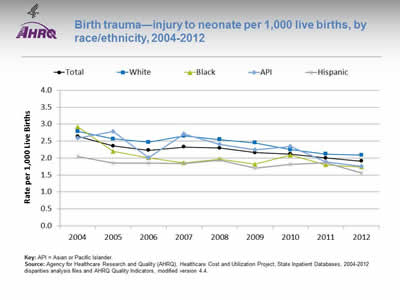
Birth trauma—injury to neonate per 1,000 live births, by race/ethnicity, 2004-2012
Image: Graph shows birth trauma—injury to neonate per 1,000 live births:
| Year | Total | White | Black | API | Hispanic |
|---|---|---|---|---|---|
| 2004 | 2.6 | 2.8 | 2.9 | 2.6 | 2.1 |
| 2005 | 2.4 | 2.6 | 2.2 | 2.8 | 1.9 |
| 2006 | 2.2 | 2.5 | 2.0 | 2.0 | 1.9 |
| 2007 | 2.3 | 2.7 | 1.9 | 2.7 | 1.8 |
| 2008 | 2.3 | 2.6 | 2.0 | 2.4 | 1.9 |
| 2009 | 2.2 | 2.5 | 1.8 | 2.2 | 1.7 |
| 2010 | 2.1 | 2.3 | 2.1 | 2.3 | 1.8 |
| 2011 | 2.0 | 2.1 | 1.8 | 1.9 | 1.9 |
| 2012 | 1.9 | 2.1 | 1.7 | 1.8 | 1.6 |
Key: API = Asian or Pacific Islander.
Source: Agency for Healthcare Research and Quality (AHRQ), Healthcare Cost and Utilization Project, State Inpatient Databases, 2004‐2012 disparities analysis files and AHRQ Quality Indicators, modified version 4.4.
Note:
- Trends:
- Birth trauma-neonatal injury rates fell from 2.6 per 1,000 live births in 2004 to 1.9 per 1,000 live births in 2012.
- Between 2004 and 2012, birth trauma-neonatal injury rates fell for all racial/ethnic groups.
- Groups With Disparities:
- In 2012, White neonates experienced an injury rate of 2.1 per 1,000 live births compared with 1.6 per 1,000 live births for Hispanic neonates.
- There were no other statistically significant differences between groups.
Part 3: Trends in Access and Priorities of the National Quality Strategy
Slide 62
National Healthcare Quality and Disparities Report Chartbook on Health Care for Hispanics
Part 3: Trends in Access and Priorities of the National Quality Strategy
Slide 63
2014 QDR Chartbooks
- 2014 QDR supported by a series of related chartbooks that:
- Present information on individual measures.
- Are updated annually.
- Are posted on the Web (http://www.ahrq.gov/research/findings/nhqrdr/2014chartbooks/).
- Order and topics of chartbooks:
- Access to care.
- Priorities of the National Quality Strategy.
- Access and quality of care for priority populations.
Note:
- Information on individual measures is available through chartbooks posted on the Web (http://www.ahrq.gov/research/findings/nhqrdr/2014chartbooks/).
Slide 64
Six Chartbooks Organized Around Priorities of the National Quality Strategy
- Making care safer by reducing harm caused in the delivery of care.
- Ensuring that each person and family is engaged as partners in their care.
- Promoting effective communication and coordination of care.
- Promoting the most effective prevention and treatment practices for the leading causes of mortality, starting with cardiovascular disease.
- Working with communities to promote wide use of best practices to enable healthy living.
- Making quality care more affordable for individuals, families, employers, and governments by developing and spreading new health care delivery models.
Slide 65
Other Chartbooks Organized Around AHRQ's Priority Populations
- AHRQ's priority populations, specified in the Healthcare Research and Quality Act of 1999 (Public Law 106-129):
- Racial and ethnic minority groups.
- Low-income groups.
- Women.
- Children (under age 18).
- Older adults (age 65 and over).
- Residents of rural areas.
- Individuals with special health care needs, including:
- Individuals with disabilities.
- Individuals who need chronic care or end-of-life care.
Slide 66

National Healthcare Quality and Disparities Report Chartbook on Health Care for Hispanics
Part 3: Trends in Access and Priorities of the National Quality Strategy
Access to Health Care
Slide 67
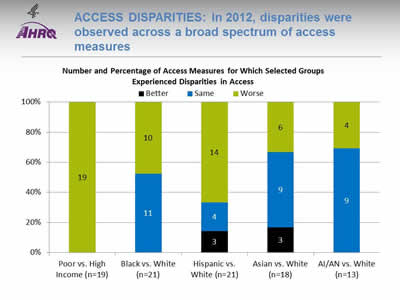
Access Disparities: In 2012, disparities were observed across a broad spectrum of access measures
Image: Chart shows Number and Percentage of Access Measures for Which Selected Groups Experienced Disparities in Access. Poor vs. High Income (n=19): Worse - 19. Black vs. White (n=21): Same - 11; Worse - 10. Hispanic vs. White (n=21): Better - 3; Same - 4; Worse - 14. Asian vs. White (n=18)): Better - 3; Same - 9; Worse - 6. AI/AN vs. White (n=13): Same - 9; Worse - 4.
- Key: AI/AN = American Indian or Alaska Native; n = number of measures.
- Note: Poor indicates family income less than the Federal poverty level; High Income indicates family income four times the Federal poverty level or greater. Numbers of measures differ across groups because of sample size limitations. Measures that achieve an overall performance level of 95% or better are not reported in the QDR and are not included in these analyses. Because disparities are typically eliminated when overall performance reaches 95%, our analyses may overstate the percentage of measures exhibiting disparities.
The relative difference between a selected group and its reference group is used to assess disparities.
- Better = Population had better access to care than reference group. Differences are statistically significant, are equal to or larger than 10%, and favor the selected group.
- Same = Population and reference group had about the same access to care. Differences are not statistically significant or are smaller than 10%.
- Worse = Population had worse access to care than reference group. Differences are statistically significant, are equal to or larger than 10%, and favor the reference group.
Example: Compared with Whites, Hispanics had worse access to care on 14 of the 21 access measures, similar access on 4 measures, and better access on 3 measures.
- Groups With Disparities:
- People in poor households experienced the largest number of disparities, followed by Hispanics and Blacks.
- In 2012, people in poor households had worse access to care than people in high-income households on all access measures (green).
- Blacks had worse access to care than Whites for about half of access measures.
- Hispanics had worse access to care than Whites for two-thirds of access measures.
- Asians and American Indians and Alaska Natives had worse access to care than Whites for about one-third of access measures.
Slide 68
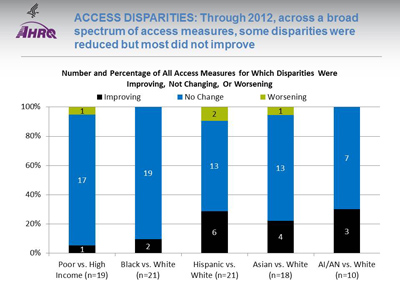
Access Disparities: Through 2012, across a broad spectrum of access measures, some disparities were reduced but most did not improve
Image: Chart shows Number and Percentage of All Access Measures for Which Disparities Were Improving, Not Changing, Or Worsening. Poor vs. High Income (n=19): Improving - 1; Not Changing - 17; Worsening - 1. Black vs. White (n=21): Improving - 2; Not Changing - 19. Hispanic vs. White (n=21): Improving - 6; Not Changing - 13; Worsening - 2. Asian vs. White (n=18): Improving - 4; Not Changing - 13; Worsening - 1. AI/AN vs. White (n=10): Improving - 3; Not Changing - 7.
Key: AI/AN = American Indian or Alaska Native; n = number of measures.
Note: Poor indicates family income less than the Federal poverty level; High Income indicates family income four times the Federal poverty level or greater. Numbers of measures differ across groups because of sample size limitations. For the vast majority of measures, trend data are available from 2001-2002 to 2012.
For each measure, average annual percentage changes were calculated for select populations and reference groups. Measures are aligned so that positive rates indicate improvement in access to care. Differences in rates between groups were used to assess trends in disparities.
- Worsening = Disparities are getting larger. Differences in rates between groups are statistically significant and reference group rates exceed population rates by at least 1% per year.
- No Change = Disparities are not changing. Differences in rates between groups are not statistically significant or differ by less than 1% per year.
- Improving = Disparities are getting smaller. Differences in rates between groups are statistically significant and population rates exceed reference group rates by at least 1% per year.
- Disparity Trends:
- Through 2012, most disparities in access to care related to race, ethnicity, or income showed no significant change (blue), neither getting smaller nor larger.
- In four of the five comparisons shown above, the number of disparities that were improving (black) exceeded the number of disparities that were getting worse (green).
Slide 69
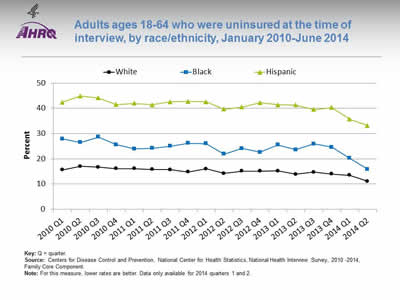
Adults ages 18-64 who were uninsured at the time of interview, by race/ethnicity, January 2010-June 2014
Image: Graph shows adults ages 18-64 who were uninsured at the time of interview:
| Quarter | Hispanic | White | Black |
|---|---|---|---|
| 2010 Q1 | 42.4 | 15.6 | 27.9 |
| 2010 Q2 | 44.9 | 17 | 26.5 |
| 2010 Q3 | 44.1 | 16.7 | 28.6 |
| 2010 Q4 | 41.5 | 16.1 | 25.6 |
| 2011 Q1 | 42 | 16.1 | 23.9 |
| 2011 Q2 | 41.4 | 15.8 | 24.2 |
| 2011 Q3 | 42.6 | 15.7 | 25 |
| 2011 Q4 | 42.7 | 14.8 | 26.2 |
| 2012 Q1 | 42.6 | 16 | 26 |
| 2012 Q2 | 39.7 | 14.2 | 21.9 |
| 2012 Q3 | 40.5 | 15.1 | 24.1 |
| 2012 Q4 | 42.2 | 15.1 | 22.6 |
| 2013 Q1 | 41.4 | 15.2 | 25.5 |
| 2013 Q2 | 41.3 | 13.9 | 23.6 |
| 2013 Q3 | 39.5 | 14.7 | 25.9 |
| 2013 Q4 | 40.3 | 14 | 24.6 |
| 2014 Q1 | 35.7 | 13.5 | 20.2 |
| 2014 Q2 | 33.2 | 11.1 | 15.9 |
Key: Q = quarter.
Source: Centers for Disease Control and Prevention, National Center for Health Statistics, National Health Interview Survey, 2010 -2014, Family Core Component.
Note: For this measure, lower rates are better. Data only available for 2014 quarters 1 and 2.
- Trends: All racial/ethnic groups displayed a decrease from 2013 Q4 to 2014 Q2:
- White: 14.0% to 11.1%.
- Black: 24.6% to 15.9%.
- Hispanic: 40.3% to 33.2%.
- Groups With Disparities: Hispanic adults ages 18-64 were significantly more likely than Whites to be uninsured from January 2010 to June 2014. The percentage peaked in the second quarter of 2010 at 44.9%, then significantly decreased to 33.2% for the second quarter of 2014.
Slide 70
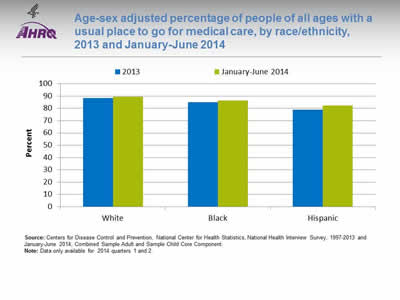
Age-sex adjusted percentage of people of all ages with a usual place to go for medical care, by race/ethnicity, 2013 and January-June 2014
Image: Chart shows age-sex adjusted percentage of people of all ages with a usual place to go for medical care. White: 2013 - 88.3; January-June 2014 - 89.3. Black: 2013 - 85; January-June 2014 - 86.5. Hispanic: 2013 - 79; January-June 2014 - 82.2.
Source: Centers for Disease Control and Prevention, National Center for Health Statistics, National Health Interview Survey, 1997-2013 and January-June 2014, Combined Sample Adult and Sample Child Core Component.
Note: Data only available for 2014 quarters 1 and 2.
- Groups With Disparities:
- From January to June 2014, after adjustment for age and sex, the percentage of people with a usual place to go for medical care was 82.2% for Hispanics, 89.3% for Whites, and 86.5% for Blacks.
- In both years, Hispanics were less likely to have a usual place to go for medical care compared with Blacks and Whites.
Slide 71
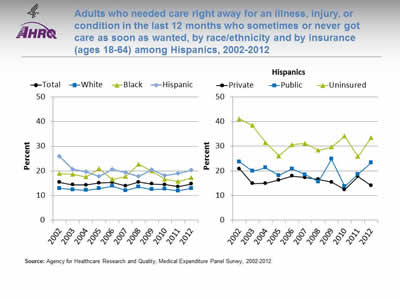
Adults who needed care right away for an illness, injury, or condition in the last 12 months who sometimes or never got care as soon as wanted, by race/ethnicity and by insurance (ages 18-64) among Hispanics, 2002-2012
Image: Graphs show adults who needed care right away for an illness, injury, or condition in the last 12 months who sometimes or never got care as soon as wanted:
Left Graph:
| Race/Ethnicity | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | 15.3 | 14.3 | 14.2 | 15.1 | 15.3 | 13.9 | 15.4 | 14.7 | 14.4 | 13.6 | 14.7 |
| Hispanic | 25.8 | 20.6 | 19.6 | 17.7 | 20.6 | 19.3 | 17.7 | 20.4 | 18.1 | 18.9 | 20.2 |
| White | 12.9 | 12.4 | 12.1 | 12.8 | 13.8 | 12 | 13.5 | 12.5 | 12.6 | 11.9 | 12.9 |
| Black | 18.9 | 18.6 | 17.5 | 20.9 | 16.5 | 17.7 | 22.7 | 19.9 | 16.6 | 15.7 | 17.2 |
Right Graph:
| Insurance | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Private | 20.8 | 14.9 | 15.0 | 16.3 | 17.9 | 17.3 | 16.6 | 15.4 | 12.4 | 17.8 | 14.1 |
| Public | 23.7 | 19.9 | 21.3 | 18.1 | 20.8 | 18.5 | 15.6 | 24.8 | 13.7 | 18.7 | 23.3 |
| Uninsured | 41.1 | 38.4 | 31.5 | 26.0 | 30.6 | 31.2 | 28.3 | 29.7 | 34.1 | 25.8 | 33.4 |
Source: Agency for Healthcare Research and Quality, Medical Expenditure Panel Survey, 2002-2012.
Note:
- Trends: From 2002 to 2012, the percentage of adults who needed care right away who sometimes or never got care as soon as wanted did not change overall or for any racial/ethnic group.
- Groups With Disparities:
- From 2010 to 2012, Hispanics were less likely than Whites to receive care as soon as wanted.
- In all years, uninsured Hispanic adults were less likely than privately insured Hispanic adults to receive needed care right away for an illness, injury, or condition in the last 12 months.
Slide 72
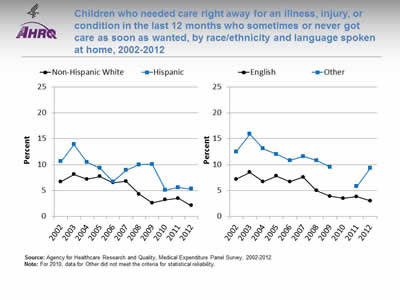
Children who needed care right away for an illness, injury, or condition in the last 12 months who sometimes or never got care as soon as wanted, by race/ethnicity and language spoken at home, 2002-2012
Image: Graphs show children who needed care right away for an illness, injury, or condition in the last 12 months who sometimes or never got care as soon as wanted:
Left Graph:
| Year | Hispanic | Non-Hispanic White |
|---|---|---|
| 2002 | 10.6 | 6.7 |
| 2003 | 13.9 | 8.1 |
| 2004 | 10.5 | 7.2 |
| 2005 | 9.3 | 7.7 |
| 2006 | 6.7 | 6.5 |
| 2007 | 8.9 | 6.8 |
| 2008 | 10.0 | 4.3 |
| 2009 | 10.1 | 2.6 |
| 2010 | 5.1 | 3.2 |
| 2011 | 5.6 | 3.5 |
| 2012 | 5.3 | 2.1 |
Right Graph:
| Year | English | Other |
|---|---|---|
| 2002 | 7.2 | 12.5 |
| 2003 | 8.5 | 15.9 |
| 2004 | 6.7 | 13.1 |
| 2005 | 7.8 | 12 |
| 2006 | 6.7 | 10.8 |
| 2007 | 7.6 | 11.6 |
| 2008 | 5 | 10.8 |
| 2009 | 3.9 | 9.5 |
| 2010 | 3.5 | |
| 2011 | 3.8 | 5.8 |
| 2012 | 3 | 9.3 |
Source: Agency for Healthcare Research and Quality, Medical Expenditure Panel Survey, 2002-2012.
Note: For 2010, data for Other did not meet the criteria for statistical reliability.
- Trends: From 2007 to 2012, Hispanic children were less likely than non-Hispanic White children to get care as soon as wanted.
- Groups With Disparities:
- In 2012, the percentage of children who needed care right away who sometimes or never got care as soon as wanted was 9.3% for those who spoke a language other than English and 3.0% for those who spoke English.
- In all years, English-speaking children were less likely than children speaking other languages to have problems receiving care as soon as wanted.
Slide 73
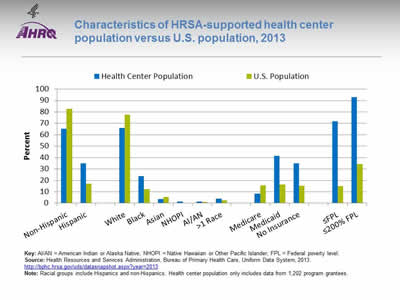
Characteristics of HRSA-supported health center population versus U.S. population, 2013
Image: Chart shows characteristics of HRSA-supported health center population versus U.S. population:
| Characteristic | Health Center Population | U.S. Population |
|---|---|---|
| Non-Hispanic | 65.2 | 82.9 |
| Hispanic | 34.8 | 17.1 |
| White | 66 | 77.7 |
| Black | 23.8 | 12.2 |
| Asian | 3.6 | 5.3 |
| NHOPI | 1.3 | 0.2 |
| AI/AN | 1.4 | 1.2 |
| >1 Race | 3.9 | 2.4 |
| Medicare | 8.4 | 15.7 |
| Medicaid | 41.5 | 16.4 |
| No Insurance | 34.9 | 15.4 |
| ≤FPL | 71.9 | 15 |
| ≤200% FPL | 92.8 | 34.2 |
Key: AI/AN = American Indian or Alaska Native; NHOPI = Native Hawaiian or Other Pacific Islander; FPL = Federal poverty level.
Source: Health Resources and Services Administration, Bureau of Primary Health Care, Uniform Data System, 2013. http://bphc.hrsa.gov/uds/datasnapshot.aspx?year=2013.
Note: Racial groups include Hispanics and non-Hispanics. Health center population only includes data from 1,202 program grantees.
- Groups With Disparities:
- In 2013, 71.9% of the health center population was at or below the Federal poverty level compared with 15% of the U.S. population. The health center population also had higher percentages of uninsurance (34.9%) and Medicaid enrollment (41.5%) than the U.S. population (15.4% and 16.4%, respectively).
- In 2013, slightly more than one-third (34.8%) of the health center population was Hispanic, which was twice as much as the percentage in the U.S. population (17.1%). The percentage of Blacks at the health centers was nearly one-quarter (23.8%), nearly twice as much as the percentage in the U.S. population (12.2%).
Slide 74
AHRQ Health Care Innovations in Access to Health Care
- Location: Primarily in rural areas of northern Colorado.
- Population: Mexican immigrants, many of whom are poor, uninsured, and monolingual with limited education.
- Intervention: Reduce health disparities by providing medical and dental care, referrals, and patient education.
- Outcomes: Enhanced access to needed medical care and education in a population who had no other way to access such services.
Slide 75

National Healthcare Quality and Disparities Report Chartbook on Health Care for Hispanics
Part 3: Trends in Access and Priorities of the National Quality Strategy
National Quality Strategy Priorities
Slide 76
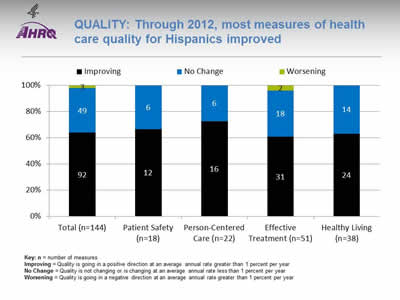
Quality: Through 2012, most measures of health care quality for Hispanics improved
Image: Chart shows measures of health care quality for Hispanics. Total (n=144): Worsening - 3; No Change - 49; Improving - 92. Patient Safety (n=18): No Change - 6; Improving - 12. Person-Centered Care (n=22): No Change - 6; Improving - 16. Effective Treatment (n=51): Worsening - 2; No Change - 18; Improving - 31. Healthy Living (n=38): No Change - 14; Improving - 24.
Key: n = number of measures
Improving = Quality is going in a positive direction at an average annual rate greater than 1 percent per year.
No Change = Quality is not changing or is changing at an average annual rate less than 1 percent per year.
Worsening = Quality is going in a negative direction at an average annual rate greater than 1 percent per year.
Note:
- Quality of care for Hispanics:
- Improved for 64% (92 out of 144) of the measures.
- Worsened for 2% (3 out of 144) of the measures.
- Did not change for 34% (49 out of 144) of the measures.
- Among the NQS priorities, quality of care for Hispanics:
- Improved for 67% (12 of 18) of Patient Safety measures and did not change for 33% (6 of 18).
- Improve for 73% (16 of 22) of Person-Centered Care measures and did not change for 27% (6 of 22).
- Improved for 61% (31 of 51) of Effective Treatment measures, worsened for 4% (2 of 51), and did not change for 35% (18 of 51).
- Improved for 63% (24 of 38) of Healthy Living measures and did not change for 37% (14 of 38).
- There are insufficient numbers of reliable measures of Care Coordination and Care Affordability to summarize in this way.
Slide 77

Quality Disparities: Disparities remained prevalent across a broad spectrum of quality measures
Image: Chart shows Number and Percentage of Quality Measures for Which Members of Selected Groups Experienced Disparities. Poor vs. High Income (n=109): Better - 6; Same - 41; Worse - 62. Black vs. White (n=165): Better - 20; Same - 85; Worse - 60. Hispanic vs. White (n=150): Better - 30; Same - 77; Worse - 43. Asian vs. White (n=146): Better - 36; Same - 78; Worse - 32. AI/AN vs. White (n=85): Better - 15; Same - 50; Worse - 20.
Key: AI/AN = American Indian or Alaska Native; n = number of measures.
Note: Poor indicates family income less than the Federal poverty level; High Income indicates family income four times the Federal poverty level or greater. Numbers of measures differ across groups because of sample size limitations. For most measures, data from 2012 are shown. Measures that achieve an overall performance level of 95% or better are not reported in the QDR and are not included in these analyses. Because disparities are typically eliminated when overall performance reaches 95%, our analyses may overstate the percentage of measures exhibiting disparities.
The relative difference between a selected group and its reference group is used to assess disparities.
- Better = Population received better quality of care than reference group. Differences are statistically significant, are equal to or larger than 10%, and favor the selected group.
- Same = Population and reference group received about the same quality of care. Differences are not statistically significant or are smaller than 10%.
- Worse = Population received worse quality of care than reference group. Differences are statistically significant, are equal to or larger than 10%, and favor the reference group.
- Groups With Disparities:
- People in poor households experienced the largest number of disparities, followed by Blacks and Hispanics.
- People in poor households received worse care than people in high-income households on more than half of quality measures (green).
- Blacks received worse care than Whites for about one-third of quality measures.
- Hispanics, American Indians and Alaska Natives, and Asians received worse care than Whites for some quality measures and better care for some measures.
- For each group, disparities in quality of care are similar to disparities in access to care, although access problems are more common than quality problems.
Slide 78
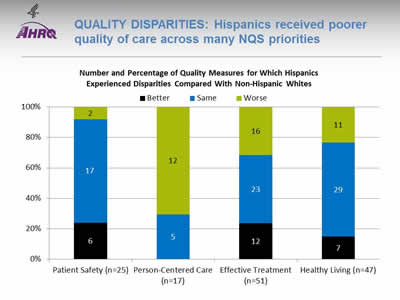
Quality Disparities: Hispanics received poorer quality of care across many NQS priorities
Image: Chart shows Number and Percentage of Quality Measures for Which Hispanics Experienced Disparities Compared With Non-Hispanic Whites. Patient Safety (n=25): Better - 6; Same - 17; Worse - 2. Person-Centered Care (n=17): Same - 5; Worse - 12. Effective Treatment (n=51): Better - 12; Same - 23; Worse - 16. Healthy Living (n=47): Better - 7; Same - 29; Worse - 11.
Key: n = number of measures.
Note: For most measures, data from 2012 are shown. Measures that achieve an overall performance level of 95% or better are not reported in the QDR and are not included in these analyses. Because disparities are typically eliminated when overall performance reaches 95%, our analyses may overstate the percentage of measures exhibiting disparities.
The relative difference between a selected group and its reference group is used to assess disparities.
- Better = Population received better quality of care than reference group. Differences are statistically significant, are equal to or larger than 10%, and favor the selected group.
- Same = Population and reference group received about the same quality of care. Differences are not statistically significant or are smaller than 10%.
- Worse = Population received worse quality of care than reference group. Differences are statistically significant, equal to or larger than 10%, and favor the reference group.
- Groups With Disparities:
- Hispanics received worse care for 70% of Person-Centered Care measures.
- Hispanics received worse care for about 30% of measures of Effective Treatment and Healthy Living.
- Hispanics received worse care for 8% of Patient Safety measures.
Slide 79
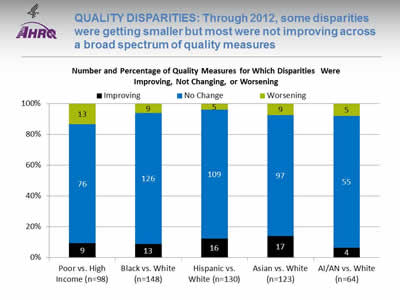
Quality Disparities: Through 2012, some disparities were getting smaller but most were not improving across a broad spectrum of quality measures
Image: Chart shows Number and Percentage of Quality Measures for Which Disparities Were Improving, Not Changing, or Worsening. Poor vs. High Income (n=98): Worsening - 13; No Change - 76; Improving - 9. Black vs. White (n=148): Worsening - 9; No Change - 126; Improving - 13. Hispanic vs. White (n=130): Worsening - 5; No Change - 109; Improving - 16. Asian vs. White (n=123): Worsening - 9; No Change - 97; Improving - 17. AI/AN vs. White (n=64): Worsening - 5; No Change - 55; Improving - 4.
Key: AI/AN = American Indian or Alaska Native; n = number of measures.
Note: Poor indicates family income less than the Federal poverty level; High Income indicates family income four times the Federal poverty level or greater. Numbers of measures differ across groups because of sample size limitations. For the majority of measures, trend data are available from 2001-2002 to 2012.
For each measure, average annual percentage changes were calculated for select populations and reference groups. Measures are aligned so that positive rates indicate improvement in access to care. Differences in rates between groups were used to assess trends in disparities.
- Worsening = Disparities are getting larger. Differences in rates between groups are statistically significant and reference group rates exceed population rates by at least 1% per year.
- No Change = Disparities are not changing. Differences in rates between groups are not statistically significant or differ by less than 1% per year.
- Improving = Disparities are getting smaller. Differences in rates between groups are statistically significant and population rates exceed reference group rates by at least 1% per year.
- Disparity Trends:
- Through 2012, most disparities in quality of care related to race, ethnicity, or income showed no significant change (blue), neither getting smaller nor larger.
- When changes in disparities occurred, measures of disparities were more likely to show improvement (black) than decline (green). However, for people in poor households, more measures showed worsening disparities than improvement.
Slide 80
Quality Disparities: Several quality measures showed elimination or widening of Hispanic-White disparities
- One quality measure showed elimination of a Hispanic-White disparity:
- Adults with obesity who ever received advice from a health professional about eating fewer high-fat foods.
- Two quality measures showed widening of Hispanic-White disparities:
- Hospice patients who received care consistent with their stated end-of-life wishes.
- Hospice patients who received the right amount of medicine for pain management.
Slide 81
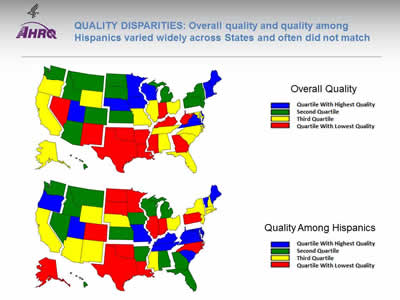
Quality Disparities: Overall quality and quality among Hispanics varied widely across States and often did not match
Image: Two maps of the United States are color-coded by state to compare overall quality and quality among Hispanics.
Source: Agency for Healthcare Research and Quality, 2014 State Snapshots.
Note: An overall quality score is computed for each State based on the number of quality measures that are above, at, or below the average across all States; States are ranked and quartiles are shown in the top map. A quality score for Hispanics is computed in a similar manner but only using data for Hispanics. Go to State Snapshots at http://nhqrnet.ahrq.gov/inhqrdr/state/select for more detailed methods.
- Geographic Disparities:
- There was significant variation in overall quality among States. States in the New England, Middle Atlantic, West North Central, and Mountain census divisions tended to have higher overall quality (blue and green) while States in the South census region tended to have lower quality (yellow and red).
- There was also significant variation among States in quality for Hispanics. Hispanics tended to receive higher quality care in States in the South Atlantic and East South Central census divisions (blue and green) and lower quality care in States in the New England, Middle Atlantic, and West South Central census divisions (yellow and red).
- The variation in State performance on overall quality and among specific priority populations may point to differential strategies for improvement. States with high overall quality but poor quality for Hispanics might target this population for support; States with low overall quality and high quality for Hispanics might seek to improve care for everyone.
- The State Snapshots tool (http://nhqrnet.ahrq.gov/inhqrdr/state/select), part of the QDR Web site, focuses on variation across States and helps State health leaders, researchers, and consumers understand the status of health care in individual States and the District of Columbia. It is based on more than 100 QDR measures for which State estimates are possible.
Slide 82
National Healthcare Quality and Disparities Report Chartbook on Health Care for Hispanics
Part 3: Trends in Access and Priorities of the National Quality Strategy
NQS Priority:Patient Safety
Slide 83
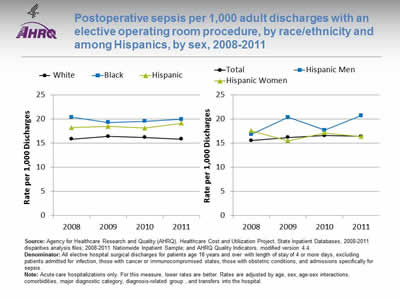
Postoperative sepsis per 1,000 adult discharges with an elective operating room procedure, by race/ethnicity and among Hispanics, by sex, 2008-2011
Image: Graphs show postoperative sepsis per 1,000 adult discharges with an elective operating room procedure:
Left Graph:
| Year | White | Hispanic | Black |
|---|---|---|---|
| 2008 | 15.9 | 18.2 | 20.4 |
| 2009 | 16.4 | 18.5 | 19.3 |
| 2010 | 16.2 | 18.2 | 19.6 |
| 2011 | 15.9 | 19.1 | 20.0 |
Right Graph:
| Year | Total | Hispanic Men | Hispanic Women |
|---|---|---|---|
| 2008 | 15.6 | 16.8 | 17.6 |
| 2009 | 16.2 | 20.4 | 15.5 |
| 2010 | 16.6 | 17.7 | 17.2 |
| 2011 | 16.4 | 20.7 | 16.4 |
Source: Agency for Healthcare Research and Quality (AHRQ), Healthcare Cost and Utilization Project, State Inpatient Databases, 2008‐2011 disparities analysis files; 2008‐2011 Nationwide Inpatient Sample; and AHRQ Quality Indicators, modified version 4.4.
Denominator: All elective hospital surgical discharges for patients age 18 years and over with length of stay of 4 or more days, excluding patients admitted for infection, those with cancer or immunocompromised states, those with obstetric conditions, and admissions specifically for sepsis.
Note: Acute care hospitalizations only. For this measure, lower rates are better. Rates are adjusted by age, sex, age-sex interactions, comorbidities, major diagnostic category, diagnosis-related group , and transfers into the hospital.
- Overall Rate: In 2011, the postoperative sepsis rate was 16.4 per 1,000 adult discharges with an elective operating room procedure.
- Trends: From 2008 through 2011, there were no statistically significant changes overall or for any racial/ethnic group in the rate of postoperative sepsis.
- Groups With Disparities:
- In all years, Hispanic patients and Black patients had higher rates of postoperative sepsis than their White counterparts.
- In 2009 and 2011, Hispanic men had higher rates of postoperative sepsis than Hispanic women.
- Groups With Disparities: From January 2009 through December 2011 combined, there were no statistically significant differences by language spoken in rates of postoperative sepsis.
Slide 84
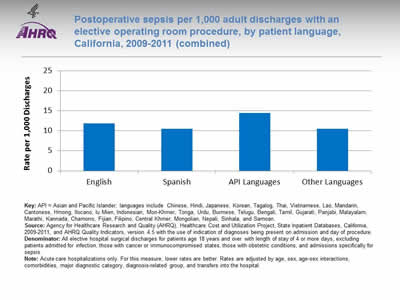
Postoperative sepsis per 1,000 adult discharges with an elective operating room procedure, by patient language, California, 2009-2011 (combined)
Image: Chart shows postoperative sepsis per 1,000 adult discharges with an elective operating room procedure by language: English - 11.84; Spanish - 10.54; API Languages - 14.44; Other Languages - 10.47.
Key: API = Asian and Pacific Islander; languages include Chinese, Hindi, Japanese, Korean, Tagalog, Thai, Vietnamese, Lao, Mandarin, Cantonese, Hmong, Ilocano, Iu Mien, Indonesian, Mon-Khmer, Tonga, Urdu, Burmese, Telugu, Bengali, Tamil, Gujarati, Panjabi, Malayalam, Marathi, Kannada, Chamorro, Fijian, Filipino, Central Khmer, Mongolian, Nepali, Sinhala, and Samoan.
Source: Agency for Healthcare Research and Quality (AHRQ), Healthcare Cost and Utilization Project, State Inpatient Databases, California, 2009-2011, and AHRQ Quality Indicators, version 4.5 with the use of indication of diagnoses being present on admission and day of procedure.
Denominator: All elective hospital surgical discharges for patients age 18 years and over with length of stay of 4 or more days, excluding patients admitted for infection, those with cancer or immunocompromised states, those with obstetric conditions, and admissions specifically for sepsis.
Note: Acute care hospitalizations only. For this measure, lower rates are better. Rates are adjusted by age, sex, age-sex interactions, comorbidities, major diagnostic category, diagnosis-related group, and transfers into the hospital.
- Groups With Disparities: From January 2009 through December 2011 combined, there were no statistically significant differences by language spoken in rates of postoperative sepsis.
Slide 85
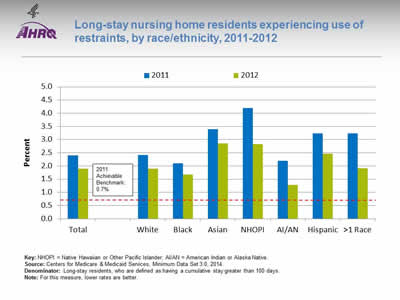
Long-stay nursing home residents experiencing use of restraints, by race/ethnicity, 2011-2012
Image: Chart shows long-stay nursing home residents experiencing use of restraints:
| Race/Ethnicity | 2011 | 2012 |
|---|---|---|
| Total | 2.4 | 1.9 |
| White | 2.4 | 1.9 |
| Black | 2.1 | 1.7 |
| Asian | 3.4 | 2.9 |
| NHOPI | 4.2 | 2.8 |
| AI/AN | 2.2 | 1.3 |
| Hispanic | 3.2 | 2.5 |
| >1 Race | 3.2 | 1.9 |
2011 Achievable Benchmark: 0.7%.
Key: NHOPI = Native Hawaiian or Other Pacific Islander; AI/AN = American Indian or Alaska Native.
Source: Centers for Medicare & Medicaid Services, Minimum Data Set 3.0, 2014.
Denominator: Long-stay residents, who are defined as having a cumulative stay greater than 100 days.
Note: For this measure, lower rates are better.
- Importance: Residents who are restrained daily can become weak, lose their ability to go to the bathroom by themselves, and develop pressure ulcers or other medical conditions.
- Overall Rate: In 2012, the percentage of long-stay nursing home residents who were physically restrained on a daily basis was 1.9%.
- Groups With Disparities:
- In 2012, Asians, Native Hawaiians and Other Pacific Islanders, and Hispanics had higher rates of daily restraint use compared with Whites.
- Blacks and American Indians and Alaska Natives had lower rates of daily restraint use compared with Whites.
- Achievable Benchmark:
- In 2011, the top 5 State achievable benchmark for restraint use was 0.7%. The States that contributed to the achievable benchmark are Kansas, Maine, Nebraska, New Hampshire, and Vermont.
- No group has achieved the benchmark.
Slide 86
National Healthcare Quality and Disparities Report Chartbook on Health Care for Hispanics
Part 3: Trends in Access and Priorities of the National Quality Strategy
NQS Priority: Person-Centered Care
Slide 87
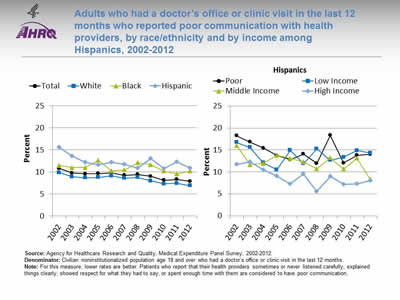
Adults who had a doctor's office or clinic visit in the last 12 months who reported poor communication with health providers, by race/ethnicity and by income among Hispanics, 2002-2012
Image: Graphs show adults who had a doctor's office or clinic visit in the last 12 months who reported poor communication with health providers:
Left Graph:
| Race/Ethnicity | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | 10.8 | 9.8 | 9.6 | 9.7 | 9.8 | 9.3 | 9.5 | 9.0 | 8.1 | 8.3 | 7.9 |
| White | 9.8 | 8.9 | 8.7 | 8.8 | 9.1 | 8.6 | 8.8 | 8.0 | 7.3 | 7.4 | 6.9 |
| Black | 11.5 | 11.0 | 11.0 | 12.7 | 10.3 | 10.5 | 12.1 | 11.7 | 10.2 | 9.6 | 10.2 |
| Hispanic | 15.6 | 13.6 | 12.2 | 11.7 | 12.2 | 11.8 | 10.9 | 13.0 | 10.8 | 12.3 | 10.9 |
Right Graph (Hispanics):
| Income | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Poor | 18.3 | 16.8 | 15.4 | 13.7 | 12.8 | 14.1 | 11.9 | 18.3 | 12.0 | 13.8 | 14.0 |
| Low Income | 16.7 | 15.6 | 12.1 | 10.5 | 14.9 | 11.9 | 15.3 | 12.7 | 13.4 | 14.9 | 14.3 |
| Middle Income | 16.0 | 11.6 | 11.9 | 13.8 | 13.1 | 12.3 | 10.7 | 13.2 | 10.6 | 13.1 | 8.3 |
| High Income | 11.7 | 12.3 | 10.5 | 9.1 | 7.3 | 9.6 | 5.6 | 9.0 | 7.2 | 7.3 | 8.0 |
Source: Agency for Healthcare Research and Quality, Medical Expenditure Panel Survey, 2002-2012.
Denominator: Civilian noninstitutionalized population age 18 and over who had a doctor's office or clinic visit in the last 12 months.
Note: For this measure, lower rates are better. Patients who report that their health providers sometimes or never listened carefully, explained things clearly, showed respect for what they had to say, or spent enough time with them are considered to have poor communication.
- Trends: From 2002 to 2012, the percentage of adults who reported poor communication with health providers significantly decreased for Whites, Hispanics, and all income groups. There were no statistically significant changes among Blacks.
- Groups With Disparities:
- In all years, Hispanics were significantly more likely than Whites to have poor communication with their health providers.
- In all years except 2006, Blacks were significantly more likely than Whites to have poor communication with their health providers.
- In all years except 2003, poor Hispanics were significantly more likely than high-income Hispanics to have poor communication with their health providers.
Slide 88
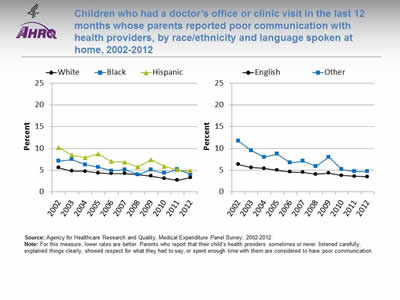
Children who had a doctor's office or clinic visit in the last 12 months whose parents reported poor communication with health providers, by race/ethnicity and language spoken at home, 2002-2012
Image: Graphs show children who had a doctor's office or clinic visit in the last 12 months whose parents reported poor communication with health providers:
Left Graph:
| Race/Ethnicity | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| White | 5.6 | 4.8 | 4.8 | 4.4 | 4.2 | 4.2 | 4.0 | 3.6 | 3.1 | 2.7 | 3.3 |
| Black | 7.1 | 7.5 | 6.3 | 5.7 | 4.8 | 5.1 | 4.0 | 5.1 | 4.3 | 5.2 | 4.1 |
| Hispanic | 10.2 | 8.4 | 7.9 | 8.8 | 7.0 | 6.8 | 5.8 | 7.4 | 5.9 | 5.1 | 4.8 |
Right Graph:
| Language | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| English | 6.3 | 5.6 | 5.4 | 5.0 | 4.6 | 4.5 | 4.1 | 4.3 | 3.8 | 3.6 | 3.5 |
| Other | 11.7 | 9.5 | 8.0 | 8.7 | 6.7 | 7.1 | 5.9 | 8.0 | 5.2 | 4.7 | 4.7 |
Source: Agency for Healthcare Research and Quality, Medical Expenditure Panel Survey, 2002-2012.
Note: For this measure, lower rates are better. Parents who report that their child's health providers sometimes or never listened carefully, explained things clearly, showed respect for what they had to say, or spent enough time with them are considered to have poor communication.
- Trends: From 2002 to 2012, the percentage of children whose parents reported poor communication with health providers significantly decreased for all racial/ethnic groups and both language groups.
- Ethnicity:
- Whites: 5.6% to 3.3%.
- Blacks: 7.1% to 4.1%.
- Hispanics: 10.2% to 4.8%.
- Preferred language:
- English: 6.3% to 3.5%.
- Other: 11.7% to 4.7%.
- Ethnicity:
- Groups With Disparities:
- In 2012, parents of Hispanic children were significantly more likely to report poor communication compared with parents of White children.
- Also in 2012, there were no statistically significant differences between Blacks and Whites or by preferred language.
Slide 89
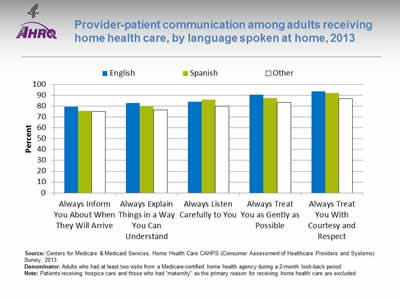
Provider-patient communication among adults receiving home health care, by language spoken at home, 2013
Image: Bar chart shows provider-patient communication among adults receiving home health care, by language spoken at home:
| Language | Always Inform You About When They Will Arrive | Always Explain Things in a Way You Can Understand | Always Listen Carefully to You | Always Treat You as Gently as Possible | Always Treat You With Courtesy and Respect |
|---|---|---|---|---|---|
| English | 79.6 | 83.1 | 84.3 | 90.7 | 93.8 |
| Other | 75.0 | 76.8 | 80.1 | 83.7 | 87.1 |
| Spanish | 75.7 | 80.4 | 86.2 | 87.5 | 92.3 |
Source: Centers for Medicare & Medicaid Services, Home Health Care CAHPS (Consumer Assessment of Healthcare Providers and Systems) Survey, 2013.
Denominator: Adults who had at least two visits from a Medicare-certified home health agency during a 2-month look-back period.
Note: Patients receiving hospice care and those who had "maternity" as the primary reason for receiving home health care are excluded
- Groups With Disparities:
- In 2013, compared with English speakers, adults speaking Spanish or another language at home were significantly less likely to:
- Always be informed about when their provider would arrive.
- Always have things explained in a way that was easy to understand.
- Always be treated as gently as possible.
- Always be treated with courtesy and respect.
- In 2013, compared with English speakers, adults speaking Spanish or another language at home were significantly less likely to:
- Adults speaking a language other than English or Spanish were significantly less likely than English- and Spanish-speaking adults to always have the provider listen carefully to them.
- Adults speaking Spanish at home were significantly more likely than English-speaking adults to report that the provider always listened carefully to them.
Slide 90
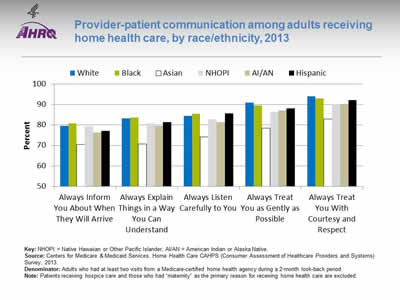
Provider-patient communication among adults receiving home health care, by race/ethnicity, 2013
Image: Bar chart shows provider-patient communication among adults receiving home health care:
| Race / Ethnicity | Always Inform You About When They Will Arrive | Always Explain Things in a Way You Can Understand | Always Listen Carefully to You | Always Treat You as Gently as Possible | Always Treat You With Courtesy and Respect |
|---|---|---|---|---|---|
| AI/AN | 76.2 | 79.5 | 81.4 | 87.2 | 90.4 |
| Asian | 70.5 | 70.7 | 74.1 | 78.4 | 83.0 |
| Black | 80.8 | 83.6 | 85.5 | 89.6 | 93.0 |
| NHOPI | 79.5 | 80.7 | 82.7 | 86.2 | 90.1 |
| White | 79.5 | 83.2 | 84.6 | 90.9 | 94.1 |
| Hispanic | 77.2 | 81.4 | 85.6 | 88.1 | 92.2 |
Key: NHOPI = Native Hawaiian or Other Pacific Islander; AI/AN = American Indian or Alaska Native.
Source: Centers for Medicare & Medicaid Services, Home Health Care CAHPS (Consumer Assessment of Healthcare Providers and Systems) Survey, 2013.
Denominator: Adults who had at least two visits from a Medicare-certified home health agency during a 2-month look-back period.
Note: Patients receiving hospice care and those who had "maternity" as the primary reason for receiving home health care are excluded.
- Groups With Disparities:
- In 2013, among home health care patients, compared with Whites:
- Asians, American Indians and Alaska Natives (AI/ANs), and Hispanics were significantly less likely to always be informed about when their provider would arrive.
- Asians, Native Hawaiians and Other Pacific Islanders (NHOPIs), AI/ANs, and Hispanics were significantly less likely to always have things explained in a way that was easy to understand.
- Asians, NHOPIs, and AI/ANs were significantly less likely to always be listened to carefully.
- Blacks, Asians, NHOPIs, AI/ANs, and Hispanics were significantly less likely to always be treated as gently as possible.
- Blacks, Asians, NHOPIs, AI/ANs, and Hispanics were significantly less likely to always be treated with courtesy and respect.
- In 2013, among home health care patients, compared with Whites:
Slide 91
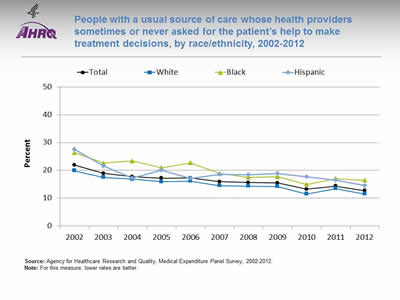
People with a usual source of care whose health providers sometimes or never asked for the patient's help to make treatment decisions, by race/ethnicity, 2002-2012
Image: Graph shows people with a usual source of care whose health providers sometimes or never asked for the patient's help to make treatment decisions:
| Race/Ethnicity | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | 21.9 | 18.9 | 17.7 | 17.2 | 17.3 | 15.9 | 15.6 | 15.4 | 13.2 | 14.3 | 12.7 |
| White | 19.9 | 17.5 | 16.8 | 15.9 | 16.1 | 14.5 | 14.3 | 14.2 | 11.5 | 13.4 | 11.5 |
| Black | 26.4 | 22.6 | 23.4 | 20.9 | 22.7 | 18.9 | 17.5 | 17.7 | 14.9 | 17 | 16.4 |
| Hispanic | 27.6 | 21.6 | 17.2 | 20 | 17 | 18.5 | 18.4 | 18.9 | 17.7 | 16.5 | 14.5 |
Source: Agency for Healthcare Research and Quality, Medical Expenditure Panel Survey, 2002-2012.
Note: For this measure, lower rates are better.
- Trends: Significant improvements were observed from 2002 to 2012:
- Total: 21.9% to 12.7%.
- Whites: 19.9% to 11.5%.
- Blacks: 26.4% to 16.4%.
- Hispanics: 27.6% to 14.5%.
- Groups With Disparities:
- In all years, Blacks were significantly less likely than Whites to be involved in their treatment decisions.
- In all years except 2004 and 2006, Hispanics were significantly less likely than Whites to be involved in their treatment decisions.
Slide 92
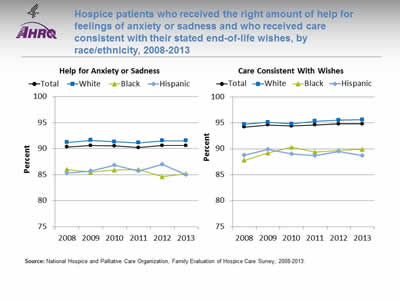
Hospice patients who received the right amount of help for feelings of anxiety or sadness and who received care consistent with their stated end-of-life wishes, by race/ethnicity, 2008-2013
Image: Graphs show hospice patients who received the right amount of help for feelings of anxiety or sadness and who received care consistent with their stated end-of-life wishes:
Left Graph (Help for Anxiety or Sadness):
| Race/Ethnicity | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 |
|---|---|---|---|---|---|---|
| Total | 90.3 | 90.6 | 90.5 | 90.2 | 90.6 | 90.6 |
| White | 91.2 | 91.6 | 91.3 | 91.1 | 91.5 | 91.5 |
| Black | 86 | 85.5 | 85.9 | 86 | 84.6 | 85.2 |
| Hispanic | 85.3 | 85.7 | 86.8 | 85.7 | 87 | 85 |
Right Graph (Care Consistent With Wishes):
| Race/Ethnicity | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 |
|---|---|---|---|---|---|---|
| Total | 94.2 | 94.6 | 94.4 | 94.6 | 94.8 | 94.8 |
| White | 94.7 | 95.1 | 94.8 | 95.3 | 95.5 | 95.6 |
| Black | 87.8 | 89.2 | 90.3 | 89.4 | 89.7 | 89.9 |
| Hispanic | 88.8 | 89.9 | 89 | 88.7 | 89.5 | 88.7 |
Source: National Hospice and Palliative Care Organization, Family Evaluation of Hospice Care Survey, 2008-2013.
Note:
- Help for Anxiety or Sadness:
- Trends: From 2008 to 2013, there were no statistically significant changes by race/ethnicity in the percentage of hospice patients who received the right amount of help for feelings of anxiety or sadness.
- Groups With Disparities: In 2013, Hispanics and Blacks were significantly less likely than Whites to receive the right amount of help for feelings of anxiety or sadness.
- Care Consistent With Stated Wishes:
- Trends: From 2008 to 2013, the percentage of hospice patients age 65 and over who received care consistent with their stated end-of-life wishes significantly improved from 94.4% to 95.1% (data not shown). From 2008 to 2013, White (94.7% to 95.6%) and Black (87.8% to 89.9%) hospice patients showed significant improvement, whereas Hispanics showed no statistically significant changes during this period.
- Groups With Disparities: In 2013, Black and Hispanic hospice patients were significantly less likely than White patients to receive care consistent with their stated end-of-life wishes.
Slide 93
AHRQ Health Care Innovations in Hospice Care
- Location: Boca Raton, Florida.
- Population: Hispanic patients and families.
- Intervention: Abriendo Puertas featured cultural competency training for all staff; a dedicated, bilingual care team; and outreach to educate local Hispanics and their physicians about the availability and purpose of hospice services.
- Outcomes: Enhanced awareness of, attitudes about, and willingness to accept hospice services among Hispanics, as well as improved cultural competency among staff.
Slide 94
National Healthcare Quality and Disparities Report Chartbook on Health Care for Hispanics
Part 3: Trends in Access and Priorities of the National Quality Strategy
NQS Priority: Care Coordination
Slide 95
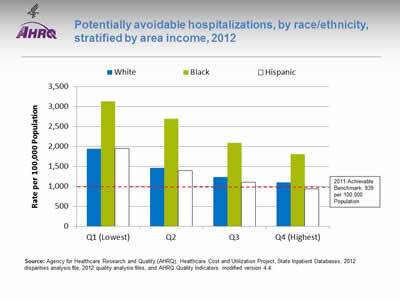
Potentially avoidable hospitalizations, by race/ethnicity, stratified by area income, 2012
Image: Chart shows potentially avoidable hospitalizations:
| Income | White | Black | Hispanic |
|---|---|---|---|
| Q1 (Lowest) | 1936 | 3131.3 | 1945.9 |
| Q2 | 1464.9 | 2694.8 | 1390.9 |
| Q3 | 1226.7 | 2091.6 | 1104.1 |
| Q4 (Highest) | 1096.5 | 1800.3 | 932 |
2011 Achievable Benchmark: 939 per 100,000 Population.
Source: Agency for Healthcare Research and Quality (AHRQ), Healthcare Cost and Utilization Project, State Inpatient Databases, 2012 disparities analysis file, 2012 quality analysis files, and AHRQ Quality Indicators, modified version 4.4.
Note:
- Groups With Disparities: In 2012, in all income groups, rates of potentially avoidable hospitalizations for all conditions were higher for Blacks than Whites.
- Achievable Benchmark:
- In 2011, the top 4 State achievable benchmark for all potentially avoidable hospitalizations was 939 per 100,000 population. %. The States that contributed to the achievable benchmark are Hawaii, Oregon, Utah, and Washington.
- The overall achievable benchmark could not be attained for 13 years.
- Hispanics in the highest income quartile have already achieved the benchmark.
Slide 96
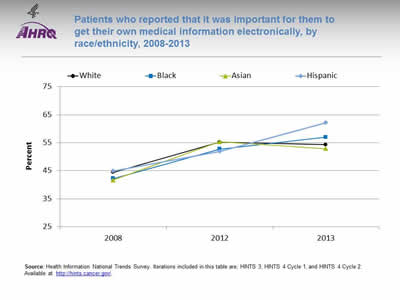
Patients who reported that it was important for them to get their own medical information electronically, by race/ethnicity, 2008-2013
Image: Graph shows patients who reported that it was important for them to get their own medical information electronically:
| Race/Ethnicity | 2008 | 2012 | 2013 |
|---|---|---|---|
| White | 44.4 | 55.2 | 54.3 |
| Black | 42.2 | 52.7 | 57 |
| Asian | 41.7 | 55.3 | 52.9 |
| Hispanic | 44.9 | 51.9 | 62.2 |
Source: Health Information National Trends Survey. Iterations included in this table are; HINTS 3, HINTS 4 Cycle 1, and HINTS 4 Cycle 2. Available at http://hints.cancer.gov/.
Note:
- Trends:
- From 2008 to 2013, the percentage of Black, White, and Hispanic patients who reported that it was very important to be able to get their medical information electronically increased significantly.
- Groups With Disparities:
- In 2013, Hispanic patients were more likely than White patients to report that it was very important to be able to get their medical information electronically.
Slide 97
AHRQ Health Care Innovations in Care Coordination
- Location: Springfield, Massachusetts.
- Population: Predominantly Latino patients with chronic illnesses and disabilities.
- Intervention: With funding from a per capita payment system, nurses at this community-based primary care clinic provide culturally competent care coordination.
- Outcomes: Improved the provision of recommended care processes, reduced health care costs, and enhanced self-management capabilities.
Slide 98

National Healthcare Quality and Disparities Report Chartbook on Health Care for Hispanics
Part 3: Trends in Access and Priorities of the National Quality Strategy
NQS Priority: Effective Treatment
- Most measures of Effective Treatment tracked in the QDR relate to priorities of the Heckler Report. Here, we illustrate effective treatment of conditions that were not priorities of the Heckler Report:
- Chronic kidney diseases.
- Musculoskeletal diseases.
- Respiratory diseases.
Slide 99
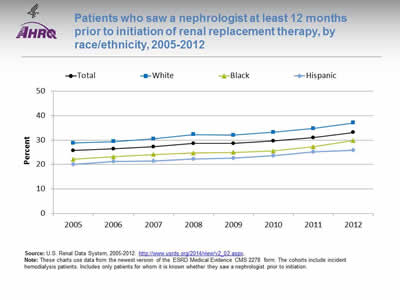
Patients who saw a nephrologist at least 12 months prior to initiation of renal replacement therapy, by race/ethnicity, 2005-2012
Image: Graph shows patients who saw a nephrologist at least 12 months prior to initiation of renal replacement therapy:
| Race/Ethnicity | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 |
|---|---|---|---|---|---|---|---|---|
| Total | 25.7 | 26.4 | 27.3 | 28.6 | 28.6 | 29.6 | 31 | 33.1 |
| Hispanic | 20 | 21.3 | 21.4 | 22.3 | 22.6 | 23.7 | 25.1 | 25.9 |
| Black | 22.2 | 23.2 | 24.1 | 24.7 | 25.0 | 25.6 | 27.3 | 29.8 |
| White | 28.8 | 29.4 | 30.5 | 32.3 | 32.0 | 33.2 | 34.7 | 37 |
Source: U.S. Renal Data System, 2005-2012. http://www.usrds.org/2014/view/v2_02.aspx.
Note: These charts use data from the newest version of the ESRD Medical Evidence CMS 2278 form. The cohorts include incident hemodialysis patients. Includes only patients for whom it is known whether they saw a nephrologist prior to initiation.
- Importance:
- Early referral to a nephrologist is important for patients with progressive chronic kidney disease who are approaching kidney failure.
- Patients who begin nephrology care more than a year before kidney failure are less likely to begin dialysis with a catheter, experience infections related to vascular access, or die during the months after dialysis initiation (USRDS, 2013*).
- Trends: The percentage of new end stage renal disease (ESRD) patients who began nephrology care at least 12 months prior to initiation of renal replacement therapy improved overall and among Whites but there were no statistically significant improvements among Hispanics and Blacks.
- Groups With Disparities: In all years, the percentage of new ESRD patients who began nephrology care at least 12 months prior to initiation of renal replacement therapy was higher Whites than for Hispanics.
* U.S. Renal Data System. USRDS 2013 annual data report: atlas of chronic kidney disease and end-stage renal disease in the United States. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2013. Available at: http://www.usrds.org/2014/view/v2_02.aspx. Accessed September 19, 2015.
Slide 100
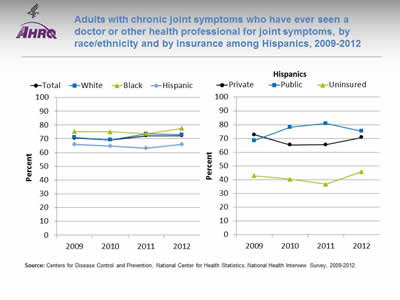
Adults with chronic joint symptoms who have ever seen a doctor or other health professional for joint symptoms, by race/ethnicity and by insurance among Hispanics, 2009-2012
Image: Graphs show adults with chronic joint symptoms who have ever seen a doctor or other health professional for joint symptoms:
Left Graph:
| Race/Ethnicity | 2009 | 2010 | 2011 | 2012 |
|---|---|---|---|---|
| Total | 70.5 | 69.1 | 72.1 | 72.1 |
| Hispanic | 65.9 | 64.7 | 63.2 | 65.9 |
| Black | 75.2 | 75.0 | 73.7 | 77.6 |
| White | 71.0 | 69.2 | 73.5 | 73.0 |
Right Graph (Hispanics):
| Insurance | 2009 | 2010 | 2011 | 2012 |
|---|---|---|---|---|
| Private | 72.7 | 65.3 | 65.5 | 70.7 |
| Public | 68.5 | 78.2 | 80.8 | 75.3 |
| Uninsured | 42.9 | 40.3 | 36.7 | 45.8 |
Source: Centers for Disease Control and Prevention, National Center for Health Statistics, National Health Interview Survey, 2009-2012.
Note:
- Trends:
- In 2012, 72.1% of adults with chronic joint symptoms reported seeing a doctor or other health professional for joint symptoms.
- There were no statistically significant improvements overall or among any racial/ethnic group.
- Groups With Disparities:
- In all years, Hispanics were less likely than Whites to report seeing a doctor or other health professional for joint symptoms.
- In all years, uninsured Hispanics were less likely than privately insured Hispanics to report seeing a doctor or other health professional for joint symptoms.
Slide 101
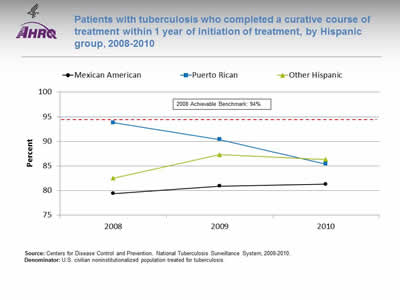
Patients with tuberculosis who completed a curative course of treatment within 1 year of initiation of treatment, by Hispanic group, 2008-2010
Image: Graph shows patients with tuberculosis who completed a curative course of treatment within 1 year of initiation of treatment:
| Hispanic Group | 2008 | 2009 | 2010 |
|---|---|---|---|
| Mexican American | 79.4 | 80.9 | 81.3 |
| Puerto Rican | 93.8 | 90.4 | 85.4 |
| Other Hispanic | 82.5 | 87.3 | 86.3 |
2008 Achievable Benchmark: 94%.
Source: Centers for Disease Control and Prevention, National Tuberculosis Surveillance System, 2008-2010.
Denominator: U.S. civilian noninstitutionalized population treated for tuberculosis.
Note:
- Groups With Disparities:
- There is considerable variation among Hispanic groups in completion of treatment for tuberculosis.
- Most groups are far from the 2008 top 4 State achievable benchmark of 94%. The States that contributed to the achievable benchmark are Colorado, Kansas, Mississippi, and Oregon.
Slide 102
National Healthcare Quality and Disparities Report Chartbook on Health Care for Hispanics
Part 3: Trends in Access and Priorities of the National Quality Strategy
NQS Priority: Healthy Living
Slide 103
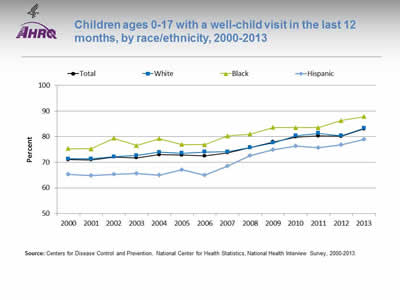
Children ages 0-17 with a well-child visit in the last 12 months, by race/ethnicity, 2000-2013
Image: Graph shows children ages 0-17 with a well-child visit in the last 12 months:
| Year | Total | White | Black | Hispanic |
|---|---|---|---|---|
| 2000 | 71.0 | 71.3 | 75.4 | 65.3 |
| 2001 | 71.0 | 71.4 | 75.2 | 64.9 |
| 2002 | 72.1 | 72.1 | 79.4 | 65.4 |
| 2003 | 71.8 | 72.7 | 76.5 | 65.6 |
| 2004 | 73.0 | 73.9 | 79.2 | 64.9 |
| 2005 | 72.8 | 73.6 | 77.0 | 67.1 |
| 2006 | 72.5 | 74.0 | 76.9 | 64.9 |
| 2007 | 73.7 | 74.1 | 80.3 | 68.5 |
| 2008 | 75.8 | 75.7 | 81.0 | 72.6 |
| 2009 | 78.0 | 77.6 | 83.6 | 74.9 |
| 2010 | 79.9 | 80.4 | 83.5 | 76.3 |
| 2011 | 80.3 | 81.3 | 83.6 | 75.8 |
| 2012 | 80.2 | 80.3 | 86.3 | 76.8 |
| 2013 | 83.0 | 83.3 | 87.8 | 79.0 |
Source: Centers for Disease Control and Prevention, National Center for Health Statistics, National Health Interview Survey, 2000-2013.
Note:
- Trends:
- Overall, the percentage of children ages 0-17 years who had a well-child visit (as distinct from a symptom-driven visit) in the last 12 months increased from 71% in 2000 to 83% in 2013.
- From 2000 to 2013, the percentage of children who had a well-child visit increased significantly for Whites (71.3% to 83.3%), Blacks (75.4% to 87.8%), and Hispanics (65.3% to 79%).
- Groups With Disparities:
- In all years, Hispanic children were less likely than White children to have had at least one well-child visit during the year.
- In all years except 2006 and 2011, Black children were more likely than White children to have at least one well-child visit.
- There were no statistically significant changes in disparities over time.
Slide 104
Prevention: Receipt of Recommended Vaccinations by Young Children
The U.S. Surgeon General, Dr. Vivek H. Murthy, and Elmo want everyone to stay healthy and get vaccinated! https://youtu.be/viS1ps0r4K0.
Slide 105
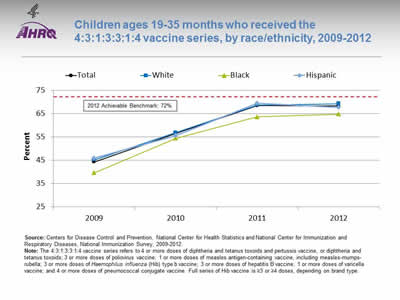
Children ages 19-35 months who received the 4:3:1:3:3:1:4 vaccine series, by race/ethnicity, 2009-2012
Image: Graph shows children ages 19-35 months who received the 4:3:1:3:3:1:4 vaccine series:
| Race/Ethnicity | 2009 | 2010 | 2011 | 2012 |
|---|---|---|---|---|
| Total | 44.3 | 56.6 | 68.5 | 68.4 |
| Hispanic | 45.9 | 55.5 | 69.5 | 67.8 |
| Black | 39.6 | 54.5 | 63.7 | 64.8 |
| White | 45.2 | 56.9 | 68.8 | 69.3 |
2012 Achievable Benchmark: 72%.
Source: Centers for Disease Control and Prevention, National Center for Health Statistics and National Center for Immunization and Respiratory Diseases, National Immunization Survey, 2009-2012.
Note: The 4:3:1:3:3:1:4 vaccine series refers to 4 or more doses of diphtheria and tetanus toxoids and pertussis vaccine, or diphtheria and tetanus toxoids; 3 or more doses of poliovirus vaccine; 1 or more doses of measles antigen-containing vaccine, including measles-mumps-rubella; 3 or more doses of Haemophilus influenza (Hib) type b vaccine; 3 or more doses of hepatitis B vaccine; 1 or more doses of varicella vaccine; and 4 or more doses of pneumococcal conjugate vaccine. Full series of Hib vaccine is ≥3 or ≥4 doses, depending on brand type.
- Trends:
- From 2009 to 2012, the percentage of children ages 19-35 months who received the 4:3:1:3:3:1:4 vaccination series improved from 44.3% to 68.4%.
- From 2009 to 2012, the percentage of children who received all recommended vaccinations improved for Blacks (39.6% to 64.8%), Hispanics (45.9% to 67.8%), and Whites (45.2% to 69.3%).
- Groups With Disparities:
- In 2012, there were no statistically significant differences between Hispanic children and White children in the percentage who received all recommended vaccines, while Black children were less likely than White children to receive all recommended vaccines.
- Achievable Benchmark:
- The 2012 top 5 State achievable benchmark was 72%. The top 5 States that contributed to the achievable benchmark are Louisiana, Maryland, Massachusetts, New Hampshire, and Ohio.
- White, Black, and Hispanic children could achieve the benchmark within a year.
Slide 106
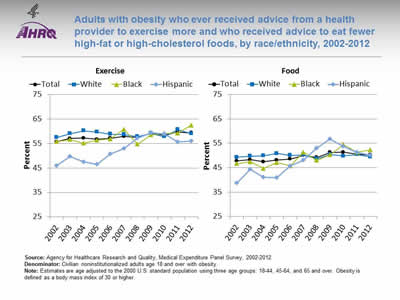
Adults with obesity who ever received advice from a health provider to exercise more and who received advice to eat fewer high-fat or high-cholesterol foods, by race/ethnicity, 2002-2012
Image: Graphs show adults with obesity who ever received advice from a health provider to exercise more and who received advice to eat fewer high-fat or high-cholesterol foods:
Left Graph (Exercise):
| Race/Ethnicity | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | 55.6 | 57.0 | 57.2 | 56.7 | 57.1 | 57.9 | 57.4 | 59.1 | 58.4 | 59.6 | 59.3 |
| White | 57.5 | 59.0 | 60.1 | 59.7 | 58.8 | 58.7 | 57.8 | 59.1 | 57.8 | 60.7 | 58.9 |
| Black | 55.8 | 56.6 | 55.1 | 56.3 | 56.8 | 60.8 | 54.7 | 58.5 | 59.1 | 59.2 | 62.4 |
| Hispanic | 45.9 | 49.7 | 47.4 | 46.5 | 50.8 | 52.8 | 57.2 | 59.4 | 58.8 | 55.7 | 55.9 |
Right Graph (Food):
| Race/Ethnicity | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | 47.7 | 48.3 | 47.4 | 48.1 | 48.5 | 50.0 | 49.2 | 51.3 | 51.4 | 50.6 | 50.2 |
| White | 49.3 | 49.7 | 49.9 | 50.9 | 50.1 | 50.2 | 48.7 | 50.4 | 49.8 | 50.4 | 49.5 |
| Black | 46.7 | 47.4 | 44.7 | 47.1 | 45.8 | 51.3 | 48.0 | 50.3 | 54.5 | 51.3 | 52.3 |
| Hispanic | 38.6 | 44.3 | 41.0 | 40.9 | 45.7 | 48.1 | 53.0 | 56.7 | 53.7 | 51.2 | 50.2 |
Source: Agency for Healthcare Research and Quality, Medical Expenditure Panel Survey, 2002-2012.
Denominator: Civilian noninstitutionalized adults age 18 and over with obesity.
Note: Estimates are age adjusted to the 2000 U.S. standard population using three age groups: 18-44, 45-64, and 65 and over. Obesity is defined as a body mass index of 30 or higher.
- Advice About Exercise:
- Overall Rate: In 2012, overall, 59.3% of adults with obesity had ever received advice from a health provider to exercise more.
- Trends: From 2002 to 2012, the percentage of obese adults who ever received advice from a health provider to exercise more improved for Blacks (from 55.8% to 62.4%) and Hispanics (from 45.9% to 55.9%).
- Groups With Disparities: In 7 of 11 years, Hispanic adults with obesity were less likely to ever receive advice from a health provider to exercise more compared with White adults with obesity. The disparity has narrowed between obese Hispanic adults and obese White adults.
- Advice About Healthy Eating:
- Overall Rate: In 2012, overall, 50.2% of adults with obesity were reported to have ever received advice from a health provider about eating fewer high-fat or high-cholesterol foods.
- Trends: From 2002 to 2012, the percentage of adults with obesity who ever received advice about healthy eating improved for Blacks (from 46.7% to 52.3%) and Hispanics (from 38.6% to 50.2%).
- Groups With Disparities: In 4 of 11 years, the percentage of Hispanic adults with obesity who ever received advice about healthy eating was lower compared with White adults with obesity. The disparity between obese Hispanic and White adults has narrowed.
Slide 107
AHRQ Health Care Innovations in Weight Management
Lutheran Family Health Centers
- Location: Brooklyn, New York.
- Population: Children in 3rd and 4th grades.
- Intervention: With its school-based health program at PS 24, developed Cuerpo Sano/Mente Sana, a 36-week weight management program.
- Outcomes: Data on the program's effectiveness are not yet available.
Slide 108
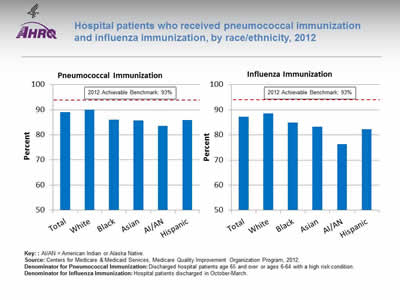
Hospital patients who received pneumococcal immunization and influenza immunization, by race/ethnicity, 2012
Image: Bar chart shows hospital patients who received pneumococcal immunization and influenza immunization. Pneumococcal Immunization: Total - 89%; White - 90.0%; Black - 86.1%; Asian - 85.7%; AI/AN - 83.5%; Hispanic - 85.8%. Influenza Immunization: Total - 87.2%; White - 88.6%; Black - 84.9%; Asian - 83.3%; AI/AN - 76.3%; Hispanic - 82.2%. 2012 Achievable Benchmark: 93%.
Key: AI/AN = American Indian or Alaska Native.
Source: Centers for Medicare & Medicaid Services, Medicare Quality Improvement Organization Program, 2012.
Denominator for Pneumococcal Immunization: Discharged hospital patients age 65 and over or ages 6-64 with a high risk condition.
Denominator for Influenza Immunization: Hospital patients discharged in October-March.
Note:
- Importance: Hospitals are important sites for ensuring people receive needed immunizations, including pneumococcal and influenza immunizations.
- Pneumococcal Immunization:
- Overall Rate: In 2012, 89% of hospital patients received pneumococcal immunization.
- Groups With Disparities: In 2012, the percentage of hospital patients who received pneumococcal immunization was lower among Blacks, Asians, AI/ANs, and Hispanics compared with Whites.
- Achievable Benchmark: The 2012 top 5 State achievable benchmark was 93%. The top 5 States that contributed to the achievable benchmark are Delaware, Florida, Ohio, South Carolina, and West Virginia. All groups were below the benchmark.
- Influenza Immunization:
- Overall Rate: in 2012, 87.2% of hospital patients received influenza immunization.
- Groups With Disparities: In 2012, the percentage of hospital patients who received influenza immunization was lower among Blacks, Asians, AI/ANs, and Hispanics compared with Whites.
- Achievable Benchmark: The 2012 top 5 State achievable benchmark was 93%. The top 5 States that contributed to the achievable benchmark are Delaware, Maryland, New Hampshire, South Carolina, and West Virginia. All groups were below the benchmark.
Slide 109
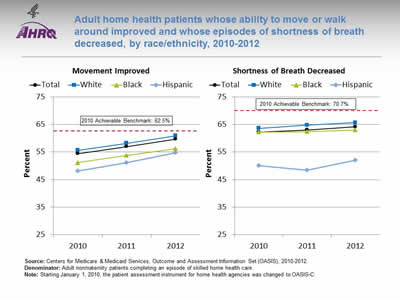
Adult home health patients whose ability to move or walk around improved and whose episodes of shortness of breath decreased, by race/ethnicity, 2010-2012
Image: Graphs show adult home health patients whose ability to move or walk around improved and whose episodes of shortness of breath decreased:
Left Graph (Movement Improved):
| Year | Total | White | Black | Hispanic |
|---|---|---|---|---|
| 2010 | 54.4 | 55.6 | 51.2 | 48.1 |
| 2011 | 57 | 58.2 | 53.8 | 51.1 |
| 2012 | 59.7 | 60.9 | 56.2 | 54.7 |
2010 Achievable Benchmark: 62.5%.
Right Graph (Shortness of Breath Decreased):
| Year | Total | White | Black | Hispanic |
|---|---|---|---|---|
| 2010 | 62.3 | 63.6 | 62.3 | 50.1 |
| 2011 | 63 | 64.8 | 62.4 | 48.4 |
| 2012 | 64.2 | 65.7 | 63 | 52 |
2010 Achievable Benchmark: 70.7%.
Source: Centers for Medicare & Medicaid Services, Outcome and Assessment Information Set (OASIS), 2010-2012.
Denominator: Adult nonmaternity patients completing an episode of skilled home health care.
Note: Starting January 1, 2010, the patient assessment instrument for home health agencies was changed to OASIS-C.
- Importance: Many patients who receive home health care are recovering from an injury or illness and may have difficulty walking or moving around safely. Maintaining and improving functional status, such as patients' ability to ambulate, improves quality of life and allows them to stay at home as long as possible. Getting better at walking or moving around may be a sign that their health status is improving. Shortness of breath interferes with activities such as walking and is an important health status indicator.
- Improved Movement:
- Overall Rate: In 2012, 59.7% of home health patients showed improvement in walking or moving around.
- Groups With Disparities: In all years, Hispanic home health patients were less likely than White home health patients to get better at walking or moving around. In 2011 and 2012, Black home health patients were less likely than White patients to get better at walking or moving around.
- Achievable Benchmark: The 2010 top 5 State achievable benchmark was 62.5%. The top 5 States that contributed to the achievable benchmark are Maine, Missouri, New Jersey, South Carolina, and Utah. No group has achieved the benchmark. Data are insufficient to determine time to benchmark.
- Decreased Shortness of Breath:
- Overall Rate: In 2012, 64.2% of home health patients had less shortness of breath.
- Groups With Disparities: In all years, Hispanics were less likely than Whites to show improvement in shortness of breath.
- Achievable Benchmark: The 2010 top 5 State achievable benchmark was 70.7%. The top 5 States that contributed to the achievable benchmark are District of Columbia, Hawaii, Maryland, New Jersey, and South Carolina. No group has achieved the benchmark. Data are insufficient to determine time to benchmark.
Slide 110
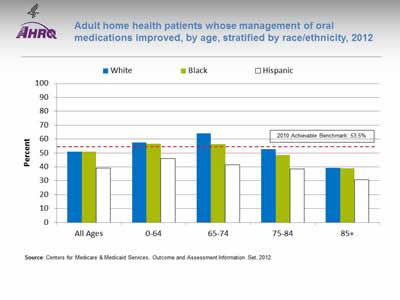
Adult home health patients whose management of oral medications improved, by age, stratified by race/ethnicity, 2012
Image: Chart shows adult home health patients whose management of oral medications improved, by age:
| Age | White | Black | Hispanic |
|---|---|---|---|
| All Ages | 50.9 | 51 | 39.2 |
| 0-64 | 57.4 | 56.6 | 45.9 |
| 65-74 | 64.1 | 56.2 | 41.4 |
| 75-84 | 52.7 | 48.4 | 38.6 |
| 85+ | 39.3 | 39 | 30.8 |
2010 Achievable Benchmark: 53.5%.
Source: Centers for Medicare & Medicaid Services, Outcome and Assessment Information Set, 2012.
Note:
- Importance: Patients who have problems taking their medications as prescribed are at risk for adverse outcomes, including lack of improvement, worsening of disease, serious side effects, and death.
- Overall Rate: In 2012, 49.7% of home health patients got better at taking their medications, compared with 47.3% in 2011 and 46.2% in 2010 (data not shown).
- Groups with Disparities: In 2012, Hispanic home health patients in all age groups were less likely than Whites and Blacks to get better at taking their medications.
- Achievable Benchmark:
- The 2010 top 5 State achievable benchmark was 53.5%. The top 5 States that contributed to the achievable benchmark are District of Columbia, Illinois, New Jersey, North Dakota, and South Carolina.
- In 2012, White and Black home health patients ages 0-64 and 65-74 had a rate higher than the benchmark.
- Data are insufficient to determine time to benchmark for other groups.
Slide 111

National Healthcare Quality and Disparities Report Chartbook on Health Care for Hispanics
Part 3: Trends in Access and Priorities of the National Quality Strategy
NQS Priority: Care Affordability
Slide 112
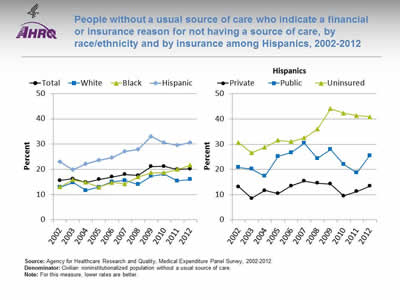
People without a usual source of care who indicate a financial or insurance reason for not having a source of care, by race/ethnicity and by insurance among Hispanics, 2002-2012
Image: Graphs show people without a usual source of care who indicate a financial or insurance reason for not having a source of care:
Left Graph:
| Race/Ethnicity | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | 15.6 | 16.3 | 14.8 | 16.0 | 17.0 | 18.0 | 17.6 | 21.1 | 21.2 | 19.9 | 20.2 |
| White | 12.8 | 14.8 | 11.6 | 13.0 | 15.1 | 15.6 | 14.0 | 17.3 | 18.0 | 15.4 | 16.0 |
| Black | 13.1 | 15.8 | 14.8 | 12.9 | 14.8 | 14.3 | 17.0 | 18.6 | 18.7 | 20.0 | 21.6 |
| Hispanic | 23.0 | 19.8 | 22.1 | 23.6 | 24.6 | 27.0 | 27.9 | 33.0 | 30.6 | 29.5 | 30.6 |
Right Graph (Hispanics):
| Insurance | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Private | 13.1 | 8.5 | 11.7 | 10.4 | 13.4 | 15.3 | 14.6 | 14.2 | 9.5 | 11.2 | 13.3 |
| Public | 20.8 | 20.2 | 17.4 | 25.2 | 26.7 | 30.4 | 24.4 | 27.9 | 22.0 | 18.7 | 25.5 |
| Uninsured | 30.6 | 26.6 | 28.8 | 31.5 | 31.0 | 32.5 | 36.0 | 44.1 | 42.4 | 41.3 | 40.9 |
Source: Agency for Healthcare Research and Quality, Medical Expenditure Panel Survey, 2002-2012.
Denominator: Civilian noninstitutionalized population without a usual source of care.
Note: For this measure, lower rates are better.
- Importance: High-quality health care is facilitated by having a regular provider, but some Americans may not be able to afford one.
- Overall Rate: In 2012, 20.2% of people without a usual source of care indicated a financial or insurance reason for not having a source of care.
- Trends:
- The overall percentage worsened from 2002 to 2010 and then leveled off.
- The percentage worsened among Blacks and Hispanics.
- Groups With Disparities: In all years, the percentage of people without a usual source of care who indicated a financial or insurance reason for not having a source of care was higher:
- Among Hispanics compared with Whites.
- Among uninsured Hispanics compared with privately insured Hispanics.
- Among publicly insured Hispanics compared with privately insured Hispanics (except in 2004).
Slide 113
AHRQ Health Care Innovations in Reducing Costs
- Location: Long Beach, California.
- Intervention: Instituted TeleSalud, a 24-hour bilingual advice line that provides callers with direct access to a registered nurse who can address their health and interpreter needs in their preferred language.
- Outcomes: Significantly increased the number of calls coming from Spanish-speaking members and has helped members to make wiser choices, leading to fewer emergency department visits and significant cost savings.
Part 4: Health Care of Residents of the U.S.-Mexico Border
Slide 114

National Healthcare Quality and Disparities Report Chartbook on Health Care for Hispanics
Part 4: Health Care of Residents of the U.S.-Mexico Border
Note:
- This part of the chartbook focuses on health care of residents on the U.S. side of the U.S.-Mexico border. In future, we will seek to add information about the Mexico side of the border.
Slide 115
U.S.-Mexico Border Region
- U.S.-Mexico border region exists within:
- 100 km (62.2 miles) of the international boundary.
- U.S. States of California, Arizona, New Mexico, and Texas.
- Mexican States of Baja California, Sonora, Chihuahua, Coahuila, Nuevo Leon, and Tamaulipas.
- U.S.-Mexico Border Health Commission focuses on border health and creates a venue to address public health along the border.
Note:
Slide 116
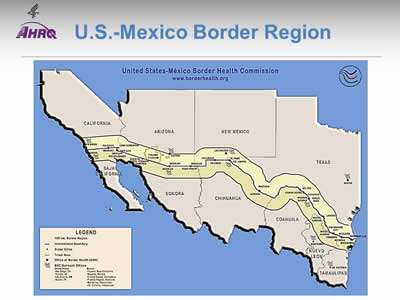
U.S.-Mexico Border Region
Image: Map shows the United States and Mexican border states: California, Arizona, New Mexico, and Texas; Baja California, Sonora, Chihuahua, Coahuila, Neuvo Leon, and Tamaulipas. The 100 km border region is highlighted.
Slide 117
Border Health Priorities
- Border health priorities include:
- Access to health care.
- Cancer.
- Environmental health.
- HIV/AIDS.
- Immunizations and infectious diseases.
- Injury prevention.
- Maternal and child health.
- Mental health.
- Oral health.
- Respiratory diseases.
Note:
Slide 118
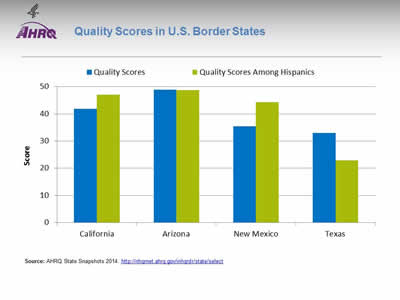
Quality Scores in U.S. Border States
Image: Chart shows Quality Scores in U.S. Border States: California Quality Scores - 41.8; Quality Scores Among Hispanics - 47.1. Arizona Quality Scores - 48.9; Quality Scores Among Hispanics - 48.8. New Mexico Quality Scores - 35.5; Quality Scores Among Hispanics - 44.3. Texas Quality Scores - 33; Quality Scores Among Hispanics - 22.9.
Source: AHRQ State Snapshots 2014. http://nhqrnet.ahrq.gov/inhqrdr/state/select.
Note:
- Methods:
- An overall quality score is computed for each State based on the number of quality measures that are above, at, or below the average across all States; the median score is typically around 50. A quality score for Hispanics is computed in a similar manner but only using data for Hispanics. Go to State Snapshots at http://nhqrnet.ahrq.gov/inhqrdr/state/select for more detailed methods.
- Geographic Variation:
- There was significant variation in overall quality among U.S. States on the border. Arizona and California are close to the median while New Mexico and Texas are far from the median, ranking 48 and 49, respectively, out of the 50 States and the District of Columbia.
- In terms of quality of care received by Hispanics, there was also significant variation among U.S. States on the border. Arizona, California, and New Mexico are close to the median while Texas ranks last out of the 50 States and the District of Columbia.
- The State Snapshots tool (http://nhqrnet.ahrq.gov/inhqrdr/state/select), part of the QDR Web site, focuses on variation across States and helps State health leaders, researchers, and consumers understand the status of health care in individual States and the District of Columbia. It is based on more than 100 QDR measures for which State estimates are possible.
Slide 119

Quality Scores in Border States by National Quality Strategy Priority
Image: Screenshot from AHRQ State Snapshots site shows Quality Scores by National Quality Strategy Priority for California, Arizona, New Mexico, and Texas.
Source: AHRQ State Snapshots 2014. http://nhqrnet.ahrq.gov/inhqrdr/state/select.
- Geographic Variation:
- Border States vary in the quality of care delivered in different priority areas of the National Quality Strategy. An overall quality score is computed for each State based on the number of quality measures that are above, at, or below the average across all States; the median score is typically around 50 and is shown as the middle of the yellow band above.
- California, Arizona, and New Mexico are weak in person-centered care. New Mexico and Texas are weak in healthy living. Texas is also weak in patient safety and care coordination. Data are limited for assessing care affordability in most States.
- Arizona is strong in care coordination.
Slide 120

Quality Scores in Border States by Condition
Image: Screenshot from AHRQ State Snapshots site shows Quality Scores by Condition for California, Arizona, New Mexico, and Texas.
Source: AHRQ State Snapshots 2014. http://nhqrnet.ahrq.gov/inhqrdr/state/select.
- Geographic Variation:
- Border States vary in the quality of care delivered for different conditions. An overall quality score is computed for each State based on the number of quality measures that are above, at, or below the average across all States; the median score is typically around 50 and is shown as the middle of the yellow band above.
- California is weak in care for chronic kidney disease. Arizona and Texas are weak in care for diabetes. Arizona and New Mexico are weak in care for mental health and substance abuse. New Mexico and Texas are weak in care for cardiovascular disease. Texas is also weak in care for HIV and AIDS.
- California, Arizona, and Texas are strong in care for cancer. Arizona and New Mexico are strong in care for HIV and AIDS. Arizona and Texas are strong in care for chronic kidney disease. Arizona is also strong in care for cardiovascular disease.
Slide 121

Quality Scores in Border States by Type of Care
Image: Screenshot from AHRQ State Snapshots site shows Quality Scores by Type of Care for California, Arizona, New Mexico, and Texas.
Source: AHRQ State Snapshots 2014. http://nhqrnet.ahrq.gov/inhqrdr/state/select.
- Geographic Variation:
- Border States vary in the quality of different types of care delivered. An overall quality score is computed for each State based on the number of quality measures that are above, at, or below the average across all States; the median score is typically around 50 and is shown as the middle of the yellow band above.
- California and New Mexico are weak in acute care. New Mexico and Texas are weak in prevention. Texas is also weak in chronic care and safety.
Slide 122
National Healthcare Quality and Disparities Report Chartbook on Health Care for Hispanics
Part 4: Health Care of Residents of the U.S.-Mexico Border
Hospital Care on the U.S.-Mexico Border
Note:
- While many of the data sources used in the QDR can provide State estimates, most cannot provide estimates at the substate level.
- In this section, we present findings from hospital data from U.S. states that can drill down to the county level. In future, we hope to identify and include data sources that can provide county estimates for care delivered in other settings.
- We also include links to some successful quality improvement interventions from the AHRQ Health Care Innovations Exchange (https://innovations.ahrq.gov/) that involved sites on the border.
Slide 123
Purpose
- Compare hospital services in counties along the U.S.-Mexico border to non-border U.S. counties in the four border States:
- AZ, CA, NM, TX.
- Focus on priority conditions identified by the U.S.-Mexico Border Commission.
- Report results by ethnicity.
Slide 124

Data Source
- Discharge counts:
- Healthcare Cost and Utilization Project:
- 2013 State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas.
- Border counties within 60 miles of Mexico.
- Discharges grouped by the county of the hospital.
- Limited to community hospitals, excluding rehabilitation hospitals.
- Included all patients treated in those hospitals, including foreign and out-of-state patients.
- Healthcare Cost and Utilization Project:
- Population denominators:
- Residents of border and non-border counties.
- Nielsen demographic data.
Slide 125
Hospital Care on the U.S.-Mexico Border
Population Characteristics
Slide 126
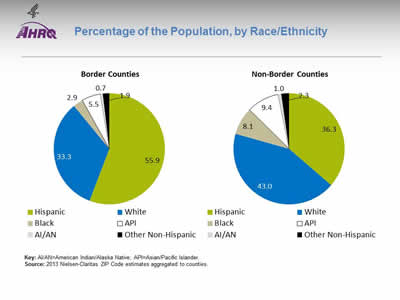
Percentage of the Population, by Race/Ethnicity
Image: Pie charts show Percentage of the Population, by Race/Ethnicity. Border Counties: Hispanic - 55.9, White - 33.3, Black - 2.9, API - 5.5, AI/AN - 0.7. Other Non-Hispanic - 1.9. Non-Border Counties: Hispanic - 36.3, White - 43.0, Black - 8.1, API - 9.4, AI/AN - 1.0, Other Non-Hispanic - 2.3.
Key: AI/AN=American Indian/Alaska Native; API=Asian/Pacific Islander.
Source: 2013 Nielsen-Claritas ZIP Code estimates aggregated to counties.
Note:
- In border counties, 56% of the population was Hispanic, compared with only 36% in non-border counties.
Slide 127
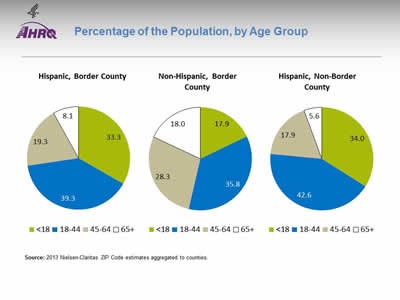
Percentage of the Population, by Age Group
Image: Pie charts show Percentage of the Population, by Age Group. Hispanic, Border County: Less than 18 - 33.3, 18-44 - 39.3, 45-64 - 19.3, 65 and over - 8.1. Non-Hispanic, Border County: Less than 18 - 17.9, 18-44 - 35.8, 45-64 - 28.3, 65 and over - 18.0. Hispanic, Non-Border County: Less than 18 - 34.0, 18-44 - 42.6, 45-64 - 17.9, 65 and over - 5.6.
Source: 2013 Nielsen-Claritas ZIP Code estimates aggregated to counties.
Note:
- The age distribution of Hispanics in border and non-border counties was similar. However, non-Hispanics in border counties were older—nearly half were age 45 and over.
Slide 128
Hospital Care on the U.S.-Mexico Border
Characteristics of Inpatient Hospital Stays
Slide 129
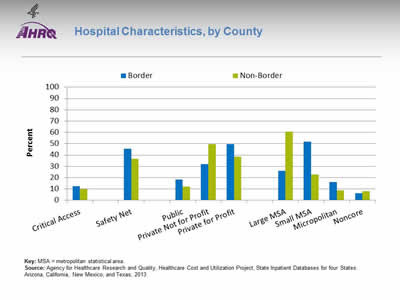
Hospital Characteristics, by County
Image: Chart shows Hospital Characteristics. Critical Access: Border - 12.3; Non-Border - 10.0. Safety Net: Border - 45.7; Non-Border - 36.8. Public: Border - 18.5; Non-Border - 12.0. Private Not for Profit: Border - 32.1; Non-Border - 49.6. Private for Profit: Border - 49.4; Non-Border - 38.4. Large MSA: Border - 25.9; Non-Border - 60.5. Small MSA: Border - 51.9; Non-Border - 22.8. Micropolitan: Border - 16.0; Non-Border - 8.9. Noncore: Border - 6.2; Non-Border - 7.9.
Key: MSA = metropolitan statistical area.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note:
- This analysis included 81 hospitals located in border counties and 789 hospitals located in the non-border counties of Arizona, California, New Mexico, and Texas.
- Compared with non-border hospitals, border hospitals were more likely to be:
- Safety net facilities.
- Public or private for profit.
- Located in small metropolitan or micropolitan areas.
Slide 130
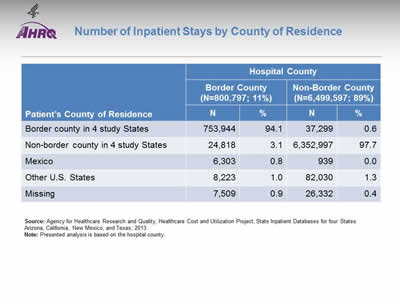
Number of Inpatient Stays by County of Residence
| Patient's County of Residence | Hospital County | |||
|---|---|---|---|---|
| Border County (N=800,797; 11%) |
Non-Border County (N=6,499,597; 89%) |
|||
| N | % | N | % | |
| Border county in 4 study States | 753,944 | 94.1 | 37,299 | 0.6 |
| Non-border county in 4 study States | 24,818 | 3.1 | 6,352,997 | 97.7 |
| Mexico | 6,303 | 0.8 | 939 | 0.0 |
| Other U.S. States | 8,223 | 1.0 | 82,030 | 1.3 |
| Missing | 7,509 | 0.9 | 26,332 | 0.4 |
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note: Presented analysis is based on the hospital county.
Slide 131
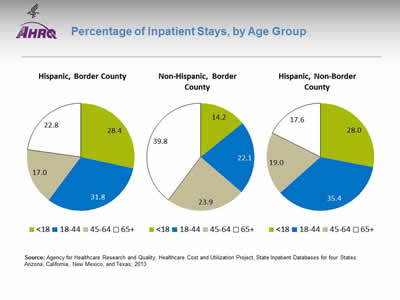
Percentage of Inpatient Stays, by Age Group
Image: Pie charts show percentage of Inpatient Stays, by Age Group. Hispanic, Border County: Less than 18 - 28.4, 18-44 - 31.8, 45-64 - 17.0, 65 and over - 22.8. Non-Hispanic, Border County: Less than 18 - 14.2, 18-44 - 22.1, 45-64 - 23.9, 65 and over - 39.8. Hispanic, Non-Border County: Less than 18 - 28.0, 18-44 - 35.4, 45-64 - 19.0, 65 and over - 17.6.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note:
- The age distribution of Hispanic inpatient stays in border and non-border counties was similar. However, non-Hispanics with an inpatient stay in border counties were older—64% were age 45 and over.
Slide 132
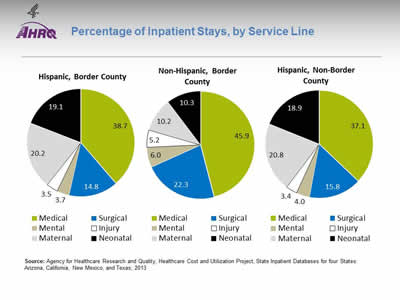
Percentage of Inpatient Stays, by Service Line
Image: Pie charts show Percentage of Inpatient Stays, by Service Line. Hispanic, Border County: Medical - 38.7, Surgical - 14.8, Mental - 3.7, Injury - 3.5, Maternal - 20.2, Neonatal - 19.1. Non-Hispanic, Border County: Medical - 45.9, Surgical - 22.3, Mental - 6.0, Injury - 5.2, Maternal - 10.2, Neonatal - 10.3. Hispanic, Non-Border County: Medical - 37.1, Surgical - 15.8, Mental - 4.0, Injury - 3.4, Maternal - 20.8, Neonatal - 18.9.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note:
- In both border and non-border counties, 40% of Hispanic inpatient stays were maternal/neonatal.
- In comparison, only 20% of non-Hispanic stays in border counties were maternal/neonatal.
Slide 133
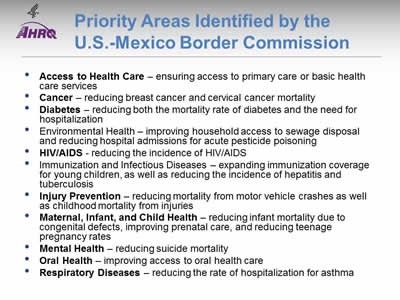
Priority Areas Identified by the U.S.-Mexico Border Commission
- Access to Health Care—ensuring access to primary care or basic health care services.
- Cancer—reducing breast cancer and cervical cancer mortality.
- Diabetes—reducing both the mortality rate of diabetes and the need for hosp.italization.
- Environmental Health—improving household access to sewage disposal and reducing hospital admissions for acute pesticide poisoning.
- HIV/AIDS—reducing the incidence of HIV/AIDS.
- Immunization and Infectious Diseases—expanding immunization coverage for young children, as well as reducing the incidence of hepatitis and tuberculosis.
- Injury Prevention—reducing mortality from motor vehicle crashes as well as childhood mortality from injuries.
- Maternal, Infant, and Child Health—reducing infant mortality due to congenital defects, improving prenatal care, and reducing teenage pregnancy rates.
- Mental Health—reducing suicide mortality.
- Oral Health—improving access to oral health care.
- Respiratory Diseases—reducing the rate of hospitalization for asthma.
Note:
Priority areas identified by Healthy Border 2010/2020. Those in bold are areas for which we provide data on subsequent slides.
Slide 134
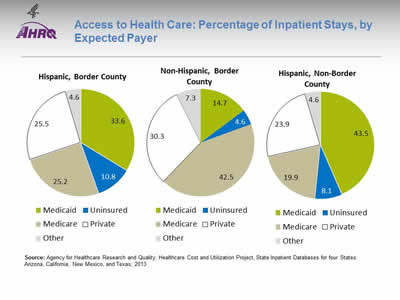
Access to Health Care: Percentage of Inpatient Stays, by Expected Payer
Image: Pie charts show Percentage of Inpatient Stays, by Expected Payer. Hispanic, Border County: Medicaid - 33.6; Uninsured - 10.8; Medicare - 25.2; Private - 25.5; Other - 4.6. Non-Hispanic, Border County: Medicaid - 14.7; Uninsured - 4.6; Medicare - 42.5; Private - 30.3; Other - 7.3. Hispanic, Non-Border County: Medicaid - 43.5; Uninsured - 8.1; Medicare - 19.9; Private - 23.9; Other - 4.6.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
- Access to health care varies by ethnicity and geographic location.
- Almost 11% of Hispanic inpatient stays in border counties were not covered by insurance, compared with:
- 4.6% of non-Hispanic stays in border counties.
- 8.1% of Hispanic stays in non-border counties.
- One-third of Hispanic inpatient stays in border counties were paid by Medicaid, compared with:
- Only 15% of non-Hispanic stays in border counties.
- About 44% of Hispanic stays in non-border counties.
Slide 135
AHRQ Health Care Innovations on the Border
- Location: Yuma County, Arizona.
- Population: Mexican farm workers.
- Intervention: Partnership between a health clinic system and a community organization, to coordinate outreach workers, known as promotoras, who help participants navigate the health care system and improve their health.
- Outcomes: Participants increased physical activity, improved dietary habits, and had higher satisfaction with their health care.
Slide 136
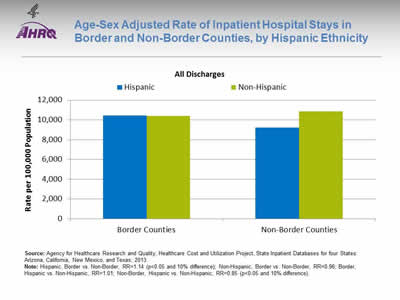
Age-Sex Adjusted Rate of Inpatient Hospital Stays in Border and Non-Border Counties, by Hispanic Ethnicity
Image: Bar chart shows rates per 100,000 population for All Discharges. Border Counties: Hispanic - 10,459; Non-Hispanic - 10,381. Non-Border Counties: Hispanic - 9,209; Non-Hispanic - 10,863.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note: Hispanic, Border vs. Non-Border, RR=1.14 (p<0.05 and 10% difference); Non-Hispanic, Border vs. Non-Border, RR=0.96; Border, Hispanic vs. Non-Hispanic, RR=1.01; Non-Border, Hispanic vs. Non-Hispanic, RR=0.85 (p<0.05 and 10% difference).
- Among Hispanics, the rate of stays was 1.14 times as high in border counties compared with non-border counties.
- In non-border counties, Hispanics had lower rates of stays than non-Hispanics.
Slide 137
Hospital Care on the U.S.-Mexico Border
Population-Based Rates of Inpatient Hospital Stays By Service Line
Slide 138
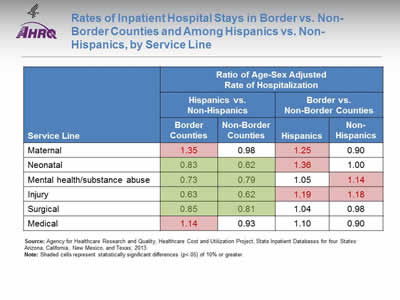
Rates of Inpatient Hospital Stays in Border vs. Non-Border Counties and Among Hispanics vs. Non-Hispanics, by Service Line
| Service Line | Ratio of Age-Sex Adjusted Rate of Hospitalization | |||
|---|---|---|---|---|
| Hispanics vs. Non-Hispanics | Border vs. Non-Border Counties | |||
| Border Counties | Non-Border Counties | Hispanics | Non-Hispanics | |
| Maternal | 1.35(a) | 0.98 | 1.25(a) | 0.90 |
| Neonatal | 0.83(b) | 0.62(b) | 1.36(a) | 1.00 |
| Mental health/substance abuse | 0.73(b) | 0.79(b) | 1.05 | 1.14(a) |
| Injury | 0.63(b) | 0.62(b) | 1.19(a) | 1.18(a) |
| Surgical | 0.85(b) | 0.81(b) | 1.04 | 0.98 |
| Medical | 1.14(a) | 0.93 | 1.10 | 0.90 |
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note: Shaded cells (a = pink, b = green) represent statistically significant differences (p<.05) of 10% or greater.
- Hispanics generally had lower rates of hospitalization than non-Hispanics, except in the medical and maternal service lines, in both border and non-border counties.
- Compared with Hispanics in non-border counties, Hispanics in border counties had higher rates of hospitalization in the injury, maternal, and neonatal service lines.
- Service lines are shown in the order they are assigned–every discharge is assigned to a hospital service line hierarchically, based on the following order: maternal and neonatal, mental health, injury, surgical, and medical. Classification for maternal and neonatal, mental health, and injury are based on the International Classification of Diseases (ICD-9-CM) principal diagnosis codes or Clinical Classifications Software (CCS). Surgical and medical splits are based on the diagnosis-related groups (DRGs). The discharge is assigned to medical if the DRG indicates ungroupable.
Slide 139
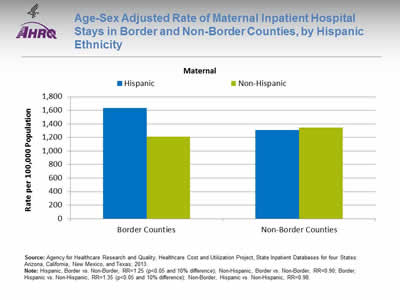
Age-Sex Adjusted Rate of Maternal Inpatient Hospital Stays in Border and Non-Border Counties, by Hispanic Ethnicity
Image: Bar chart shows rates per 100,000 population for Maternal Inpatient Hospital Stays. Border Counties: Hispanic - 1,637; Non-Hispanic - 1,211. Non-Border Counties: Hispanic - 1,311; Non-Hispanic - 1,343.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note: Hispanic, Border vs. Non-Border, RR=1.25 (p<0.05 and 10% difference); Non-Hispanic, Border vs. Non-Border, RR=0.90; Border, Hispanic vs. Non-Hispanic, RR=1.35 (p<0.05 and 10% difference); Non-Border, Hispanic vs. Non-Hispanic, RR=0.98.
- Hispanics in border counties had higher rates of maternal stays compared with both:
- Hispanics in non-border counties and
- Non-Hispanics in border counties.
Slide 140
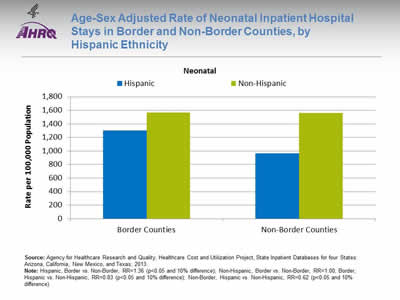
Age-Sex Adjusted Rate of Neonatal Inpatient Hospital Stays in Border and Non-Border Counties, by Hispanic Ethnicity
Image: Bar chart shows rates per 100,000 population for Neonatal Inpatient Hospital Stays. Border Counties: Hispanic - 1,304; Non-Hispanic - 1,565. Non-Border Counties: Hispanic - 963; Non-Hispanic - 1,560.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note: Hispanic, Border vs. Non-Border, RR=1.36 (p<0.05 and 10% difference); Non-Hispanic, Border vs. Non-Border, RR=1.00; Border, Hispanic vs. Non-Hispanic, RR=0.83 (p<0.05 and 10% difference); Non-Border, Hispanic vs. Non-Hispanic, RR=0.62 (p<0.05 and 10% difference).
- Among Hispanics, the rate of neonatal stays was higher in border counties than in non-border counties.
- Hispanics had lower rates of neonatal stays than non-Hispanics, both in border and non-border counties.
Slide 141
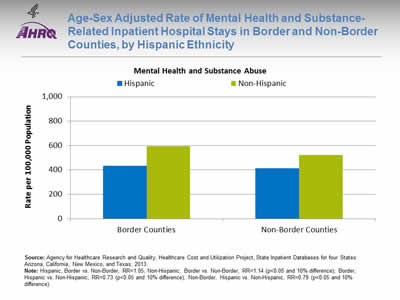
Age-Sex Adjusted Rate of Mental Health and Substance-Related Inpatient Hospital Stays in Border and Non-Border Counties, by Hispanic Ethnicity
Image: Bar chart shows rates per 100,000 population for Mental Health and Substance Abuse. Border Counties: Hispanic - 435; Non-Hispanic - 595. Non-Border Counties: Hispanic - 414; Non-Hispanic - 524.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note: Hispanic, Border vs. Non-Border, RR=1.05; Non-Hispanic, Border vs. Non-Border, RR=1.14 (p<0.05 and 10% difference); Border, Hispanic vs. Non-Hispanic, RR=0.73 (p<0.05 and 10% difference); Non-Border, Hispanic vs. Non-Hispanic, RR=0.79 (p<0.05 and 10% difference).
- Hispanics had lower rates of mental health and substance-related stays than non-Hispanics, both in border and non-border counties.
- Among non-Hispanics, those in border counties had higher rates of mental health and substance-related stays than non-Hispanics in non-border counties.
Slide 142
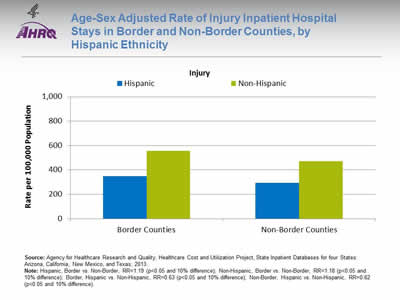
Age-Sex Adjusted Rate of Injury Inpatient Hospital Stays in Border and Non-Border Counties, by Hispanic Ethnicity
Image: Bar chart shows rates per 100,000 population for Injury. Border Counties: Hispanic - 348; Non-Hispanic - 566. Non-Border Counties: Hispanic - 293; Non-Hispanic - 471.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note: Hispanic, Border vs. Non-Border, RR=1.19 (p<0.05 and 10% difference); Non-Hispanic, Border vs. Non-Border, RR=1.18 (p<0.05 and 10% difference); Border, Hispanic vs. Non-Hispanic, RR=0.63 (p<0.05 and 10% difference); Non-Border, Hispanic vs. Non-Hispanic, RR=0.62 (p<.05 and 10% difference).
- Rates of injury stays were higher in border than non-border counties, both for Hispanics and non-Hispanics.
- Rates of injury stays were lower among Hispanics than non-Hispanics, both in border and non-border counties.
Slide 143
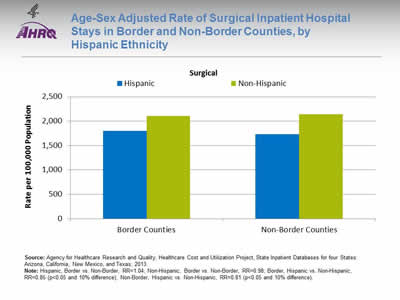
Age-Sex Adjusted Rate of Surgical Inpatient Hospital Stays in Border and Non-Border Counties, by Hispanic Ethnicity
Image: Bar chart shows rates per 100,000 population for Surgical Inpatient Hospital Stays. Border Counties: Hispanic - 1,801; Non-Hispanic - 2,109. Non-Border Counties: Hispanic - 1,730; Non-Hispanic - 2,144.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note: Hispanic, Border vs. Non-Border, RR=1.04; Non-Hispanic, Border vs. Non-Border, RR=0.98; Border, Hispanic vs. Non-Hispanic, RR=0.85 (p<0.05 and 10% difference); Non-Border, Hispanic vs. Non-Hispanic, RR=0.81 (p<0.05 and 10% difference).
- Hispanics had lower rates of surgical stays, both in border and non-border counties.
Slide 144
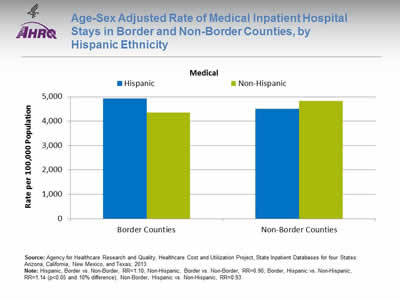
Age-Sex Adjusted Rate of Medical Inpatient Hospital Stays in Border and Non-Border Counties, by Hispanic Ethnicity
Image: Bar chart shows rates per 100,000 population for Medical Inpatient Hospital Stays. Border Counties: Hispanic - 4,933; Non-Hispanic - 4,345. Non-Border Counties: Hispanic - 4,498; Non-Hispanic - 4,822.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note: Hispanic, Border vs. Non-Border, RR=1.10; Non-Hispanic, Border vs. Non-Border, RR=0.90; Border, Hispanic vs. Non-Hispanic, RR=1.14 (p<0.05 and 10% difference); Non-Border, Hispanic vs. Non-Hispanic, RR=0.93.
- In border counties, Hispanics had higher rates of medical stays than non-Hispanics.
Slide 145
Hospital Care on the U.S.-Mexico Border
Population-Based Rates of Inpatient Hospital Stays for Select Conditions
Slide 146
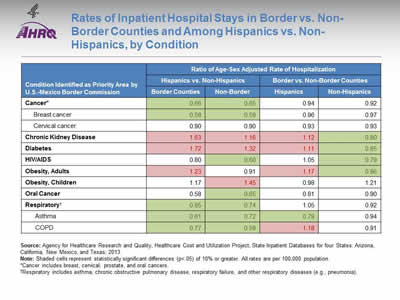
Rates of Inpatient Hospital Stays in Border vs. Non-Border Counties and Among Hispanics vs. Non-Hispanics, by Condition
| Condition Identified as Priority Area by U.S.-Mexico Border Commission | Ratio of Age-Sex Adjusted Rate of Hospitalization | |||
|---|---|---|---|---|
| Hispanics vs. Non-Hispanics | Border vs. Non-Border Counties | |||
| Border Counties | Non-Border | Hispanics | Non-Hispanics | |
| Cancer* | 0.66(b) | 0.65(b) | 0.94 | 0.92 |
| Breast cancer | 0.58(b) | 0.59(b) | 0.96 | 0.97 |
| Cervical cancer | 0.90 | 0.90 | 0.93 | 0.93 |
| Chronic Kidney Disease | 1.63(a) | 1.16(a) | 1.12(a) | 0.80(b) |
| Diabetes | 1.72(a) | 1.32(a) | 1.11(a) | 0.85(b) |
| HIV/AIDS | 0.80 | 0.60(b) | 1.05 | 0.79(b) |
| Obesity, Adults | 1.23(a) | 0.91 | 1.17(a) | 0.86(b) |
| Obesity, Children | 1.17 | 1.45(a) | 0.98 | 1.21 |
| Oral Cancer | 0.58 | 0.65(b) | 0.81 | 0.90 |
| Respiratory† | 0.85(b) | 0.74(b) | 1.05 | 0.92 |
| Asthma | 0.61(b) | 0.72(b) | 0.79(b) | 0.94 |
| COPD | 0.77(b) | 0.59(b) | 1.18(a) | 0.91 |
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note: Shaded cells (a = pink, b = green) represent statistically significant differences (p<.05) of 10% or greater. All rates are per 100,000 population.
*Cancer includes breast, cervical, prostate, and oral cancers.
†Respiratory includes asthma, chronic obstructive pulmonary disease, respiratory failure, and other respiratory diseases (e.g., pneumonia).
Slide 147
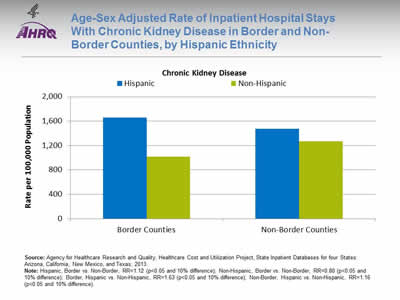
Age-Sex Adjusted Rate of Inpatient Hospital Stays With Chronic Kidney Disease in Border and Non-Border Counties, by Hispanic Ethnicity
Image: Bar chart shows rates per 100,000 population for Chronic Kidney Disease. Border Counties: Hispanic - 1,658; Non-Hispanic - 1,015. Non-Border Counties: Hispanic - 1,475; Non-Hispanic - 1,268.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note: Hispanic, Border vs. Non-Border, RR=1.12 (p<0.05 and 10% difference); Non-Hispanic, Border vs. Non-Border, RR=0.80 (p<0.05 and 10% difference); Border, Hispanic vs. Non-Hispanic, RR=1.63 (p<0.05 and 10% difference); Non-Border, Hispanic vs. Non-Hispanic, RR=1.16 (p<0.05 and 10% difference).
- For Hispanics in border counties, the rate of inpatient stays with chronic kidney disease was:
- 1.12 times as high as Hispanics in non-border counties.
- 1.63 times as high as non-Hispanics in border counties.
- Hispanics also had higher rates of chronic kidney disease in non-border counties, compared with non-Hispanics in non-border counties.
- Among non-Hispanics, those in border counties had lower rates of chronic kidney disease than those in non-border counties.
Slide 148
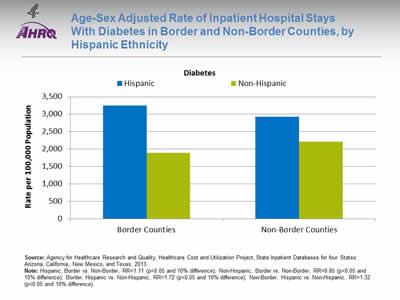
Age-Sex Adjusted Rate of Inpatient Hospital Stays With Diabetes in Border and Non-Border Counties, by Hispanic Ethnicity
Image: Bar chart shows rates per 100,000 population for Diabetes. Border Counties: Hispanic - 3,246; Non-Hispanic - 1,888. Non-Border Counties: Hispanic - 2,922; Non-Hispanic - 2,213.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note: Hispanic, Border vs. Non-Border, RR=1.11 (p<0.05 and 10% difference); Non-Hispanic, Border vs. Non-Border, RR=0.85 (p<0.05 and 10% difference); Border, Hispanic vs. Non-Hispanic, RR=1.72 (p<0.05 and 10% difference); Non-Border, Hispanic vs. Non-Hispanic, RR=1.32 (p<0.05 and 10% difference).
- For Hispanics in border counties, the rate of inpatient stays with diabetes was:
- 1.11 times as high as Hispanics in non-border counties.
- 1.72 times as high as non-Hispanics in border counties.
- Hispanics had higher rates of stays with diabetes than non-Hispanics, both in border and non-border counties.
- Among non-Hispanics, those in border counties had lower rates of stays with diabetes than those in non-border counties.
Slide 149
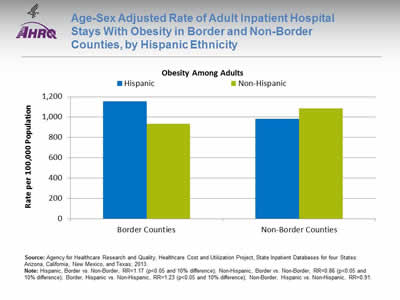
Age-Sex Adjusted Rate of Adult Inpatient Hospital Stays With Obesity in Border and Non-Border Counties, by Hispanic Ethnicity
Image: Bar chart shows rates per 100,000 population for Obesity Among Adults. Border Counties: Hispanic - 1,153; Non-Hispanic - 934. Non-Border Counties: Hispanic - 983; Non-Hispanic - 1,085.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note: Hispanic, Border vs. Non-Border, RR=1.17 (p<0.05 and 10% difference); Non-Hispanic, Border vs. Non-Border, RR=0.86 (p<0.05 and 10% difference); Border, Hispanic vs. Non-Hispanic, RR=1.23 (p<0.05 and 10% difference); Non-Border, Hispanic vs. Non-Hispanic, RR=0.91.
- For Hispanics in border counties, the rate of inpatient stays with adult obesity was:
- 1.17 times as high as Hispanics in non-border counties.
- 1.23 times as high as non-Hispanics in border counties.
- Among non-Hispanics, those in border counties had lower rates of adult obesity than those in non-border counties.
Slide 150
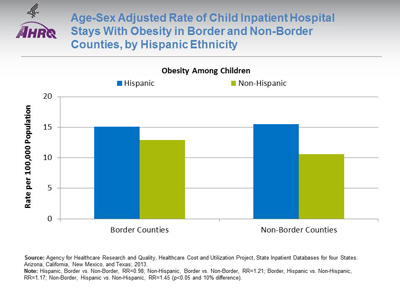
Age-Sex Adjusted Rate of Child Inpatient Hospital Stays With Obesity in Border and Non-Border Counties, by Hispanic Ethnicity
Image: Bar chart shows rates per 100,000 population for Obesity Among Children. Border Counties: Hispanic - 15.1; Non-Hispanic - 12.9. Non-Border Counties: Hispanic - 15.5; Non-Hispanic - 10.6.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note: Hispanic, Border vs. Non-Border, RR=0.98; Non-Hispanic, Border vs. Non-Border, RR=1.21; Border, Hispanic vs. Non-Hispanic, RR=1.17; Non-Border, Hispanic vs. Non-Hispanic, RR=1.45 (p<0.05 and 10% difference).
- In non-border counties, Hispanics had higher rates of child obesity than non-Hispanics.
Slide 151
AHRQ Health Care Innovations on the Border
- Location: Laredo, Texas, and Ciudad Victoria, Tamaulipas.
- Population: Mexican-American and other at-risk youth.
- Intervention: Comprehensive and culturally competent school-based behavior modification program intended to prevent or delay the onset of type 2 diabetes.
- Outcomes: Reduced risk factors, including body mass index, percentage of children with waist circumference at or above the 90th percentile, fasting insulin levels, and prevalence of obesity.
Slide 152
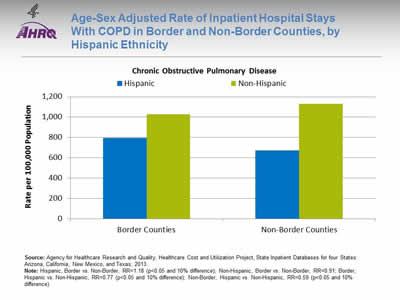
Age-Sex Adjusted Rate of Inpatient Hospital Stays With COPD in Border and Non-Border Counties, by Hispanic Ethnicity
Image: Bar chart shows rates per 100,000 population for Chronic Obstructive Pulmonary Disease. Border Counties: Hispanic - 793; Non-Hispanic - 1,027. Non-Border Counties: Hispanic - 672; Non-Hispanic - 1,132.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note: Hispanic, Border vs. Non-Border, RR=1.18 (p<0.05 and 10% difference); Non-Hispanic, Border vs. Non-Border, RR=0.91; Border, Hispanic vs. Non-Hispanic, RR=0.77 (p<0.05 and 10% difference); Non-Border, Hispanic vs. Non-Hispanic, RR=0.59 (p<0.05 and 10% difference).
- Among Hispanics, those in border counties had higher rates of COPD than those in non-border counties.
- Hispanics had lower rates of COPD than non-Hispanics, both in border and non-border counties.
Slide 153
AHRQ Health Care Innovations on the Border
El Rio Inner-City Asthma Intervention
- Location: Tucson, Arizona.
- Population: Low-income, inner-city Latino children with moderate or severe persistent asthma.
- Intervention: Comprehensive bilingual, bicultural program.
- Outcomes: Significantly reduced asthma-related emergency department visits, hospitalizations, missed school days, and sick days.
Slide 154
Hospital Care on the U.S.-Mexico Border
Complications of Inpatient Hospitals Stays with Diabetes
Slide 155
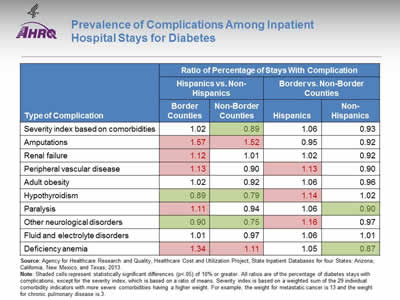
Prevalence of Complications Among Inpatient Hospital Stays for Diabetes
| Type of Complication | Ratio of Percentage of Stays With Complication | |||
|---|---|---|---|---|
| Hispanics vs. Non-Hispanics | Border vs. Non-Border Counties | |||
| Border Counties | Non-Border | Hispanics | Non-Hispanics | |
| Severity index based on comorbidities | 1.02 | 0.89(b) | 1.06 | 0.93 |
| Amputations | 1.57(a) | 1.52(a) | 0.95 | 0.92 |
| Renal failure | 1.12(a) | 1.01 | 1.02 | 0.92 |
| Peripheral vascular disease | 1.13(a) | 0.90 | 1.13(a) | 0.90 |
| Adult obesity | 1.02 | 0.92 | 1.06 | 0.96 |
| Hypothyroidism | 0.89(b) | 0.79(b) | 1.14(a) | 1.02 |
| Paralysis | 1.11(a) | 0.94 | 1.06 | 0.90(b) |
| Other neurologic disorders | 0.90(b) | 0.75(b) | 1.16(a) | 0.97 |
| Fluid and electrolyte disorders | 1.01 | 0.97 | 1.06 | 1.01 |
| Deficiency anemia | 1.34(a) | 1.11(a) | 1.05 | 0.87(b) |
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note: Shaded cells (a = pink, b = green) represent statistically significant differences (p<.05) of 10% or greater. All ratios are of the percentage of diabetes stays with complications, except for the severity index, which is based on a ratio of means. Severity index is based on a weighted sum of the 29 individual comorbidity indicators with more severe comorbidities having a higher weight. For example, the weight for metastatic cancer is 13 and the weight for chronic pulmonary disease is 3.
- Compared with non-Hispanics, Hispanics generally had higher rates of complications associated with diabetes, especially in border counties.
- Among Hispanics, those in border counties had higher rates of complications associated with diabetes compared with non-border counties.
Slide 156
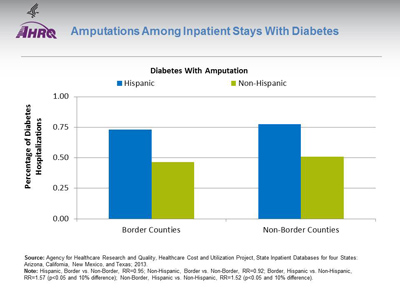
Amputations Among Inpatient Stays With Diabetes
Image: Bar chart shows percentage of hospitalizations for diabetes with amputation. Border Counties: Hispanic - 0.73; Non-Hispanic - 0.47. Non-Border Counties: Hispanic - 0.78; Non-Hispanic - 0.51.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note: Hispanic, Border vs. Non-Border, RR=0.95; Non-Hispanic, Border vs. Non-Border, RR=0.92; Border, Hispanic vs. Non-Hispanic, RR=1.57 (p<0.05 and 10% difference); Non-Border, Hispanic vs. Non-Hispanic, RR=1.52 (p<0.05 and 10% difference).
- Hispanics with diabetes were more likely to have an amputation compared with non-Hispanics with diabetes, both in border and non-border counties.
Slide 157
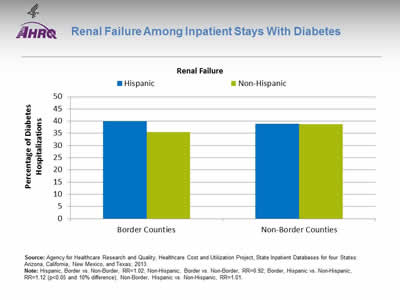
Renal Failure Among Inpatient Stays With Diabetes
Image: Bar chart shows percentage of hospitalizations for diabetes with renal failure. Border Counties: Hispanic - 39.9; Non-Hispanic - 35.5. Non-Border Counties: Hispanic - 39.0; Non-Hispanic - 38.7.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note: Hispanic, Border vs. Non-Border, RR=1.02; Non-Hispanic, Border vs. Non-Border, RR=0.92; Border, Hispanic vs. Non-Hispanic, RR=1.12 (p<0.05 and 10% difference); Non-Border, Hispanic vs. Non-Hispanic, RR=1.01.
- A higher percentage of Hispanics in border counties with an inpatient stay for diabetes had renal failure (listed as any diagnosis), compared with non-Hispanics in border counties.
Slide 158
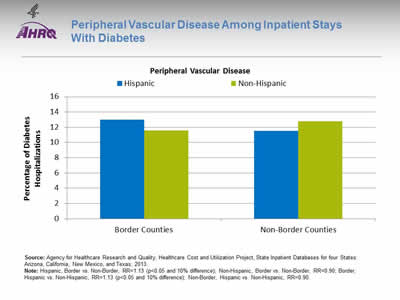
Peripheral Vascular Disease Among Inpatient Stays With Diabetes
Image: Bar chart shows percentage of hospitalizations for diabetes with peripheral vascular disease. Border Counties: Hispanic - 13.0; Non-Hispanic - 11.6. Non-Border Counties: Hispanic - 11.5; Non-Hispanic - 12.8.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note: Hispanic, Border vs. Non-Border, RR=1.13 (p<0.05 and 10% difference); Non-Hispanic, Border vs. Non-Border, RR=0.90; Border, Hispanic vs. Non-Hispanic, RR=1.13 (p<0.05 and 10% difference); Non-Border, Hispanic vs. Non-Hispanic, RR=0.90.
- A higher percentage of Hispanics in border counties with an inpatient stay for diabetes had peripheral vascular disease, compared with:
- Non-Hispanics in border counties.
- Hispanics in non-border counties.
Slide 159
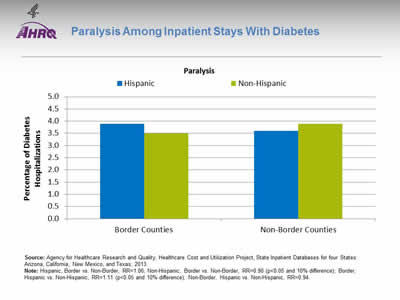
Paralysis Among Inpatient Stays With Diabetes
Image: Bar chart shows percentage of hospitalizations for diabetes with paralysis. Border Counties: Hispanic - 3.9; Non-Hispanic - 3.5. Non-Border Counties: Hispanic - 3.6; Non-Hispanic - 3.9.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note: Hispanic, Border vs. Non-Border, RR=1.06; Non-Hispanic, Border vs. Non-Border, RR=0.90 (p<0.05 and 10% difference); Border, Hispanic vs. Non-Hispanic, RR=1.11 (p<0.05 and 10% difference); Non-Border, Hispanic vs. Non-Hispanic, RR=0.94.
- Among non-Hispanics with diabetes, those in border counties had a lower prevalence of paralysis than those in non-border counties.
- In border counties, Hispanics with diabetes had a higher prevalence of paralysis than non-Hispanics with diabetes.
Slide 160
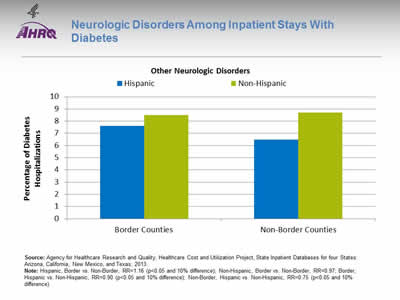
Neurologic Disorders Among Inpatient Stays With Diabetes
Image: Bar chart shows percentage of hospitalizations for diabetes with other neurologic disorders. Border Counties: Hispanic - 7.6; Non-Hispanic - 8.5. Non-Border Counties: Hispanic - 6.5; Non-Hispanic - 8.7.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note: Hispanic, Border vs. Non-Border, RR=1.16 (p<0.05 and 10% difference); Non-Hispanic, Border vs. Non-Border, RR=0.97; Border, Hispanic vs. Non-Hispanic, RR=0.90 (p<0.05 and 10% difference); Non-Border, Hispanic vs. Non-Hispanic, RR=0.75 (p<0.05 and 10% difference).
- A higher percentage of Hispanics in border counties with an inpatient stay for diabetes had neurologic disorders, compared with Hispanics in non-border counties.
- Hispanics with diabetes had lower rates of neurologic disorders than non-Hispanics with diabetes, both in border and non-border counties.
Slide 161
Hospital Care on the U.S.-Mexico Border
Complications Among Inpatient Hospital Stays For Mental Health or Substance Abuse
Slide 162
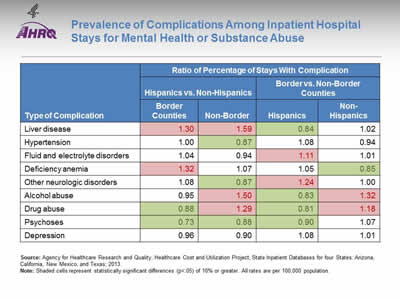
Prevalence of Complications Among Inpatient Hospital Stays for Mental Health or Substance Abuse
| Type of Complication | Ratio of Percentage of Stays With Complication | |||
|---|---|---|---|---|
| Hispanics vs. Non-Hispanics | Border vs. Non-Border Counties | |||
| Border Counties | Non-Border | Hispanics | Non-Hispanics | |
| Liver disease | 1.30(a) | 1.59(a) | 0.84(b) | 1.02 |
| Hypertension | 1.00 | 0.87(b) | 1.08 | 0.94 |
| Fluid and electrolyte disorders | 1.04 | 0.94 | 1.11(a) | 1.01 |
| Deficiency anemia | 1.32(a) | 1.07 | 1.05 | 0.85(b) |
| Other neurologic disorders | 1.08 | 0.87(b) | 1.24(a) | 1.00 |
| Alcohol abuse | 0.95 | 1.50(a) | 0.83(b) | 1.32(a) |
| Drug abuse | 0.88(b) | 1.29(a) | 0.81(b) | 1.18(a) |
| Psychoses | 0.73(b) | 0.88(b) | 0.90(b) | 1.07 |
| Depression | 0.96 | 0.90 | 1.08 | 1.01 |
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note: Shaded cells (a = pink, b = green) represent statistically significant differences (p<.05) of 10% or greater. All rates are per 100,000 population.
- Compared with non-Hispanics, Hispanics were more likely to have a code for liver disease, both in border and non-border counties.
- Among Hispanics, compared with those in non-border counties, those in border counties were:
- Less likely to have a code for liver disease, alcohol and drug abuse, and psychoses.
- More likely to have fluid and electrolyte disorders and other neurologic disorders.
- Among non-Hispanics, those in border counties were more likely to have a code for drug or alcohol abuse than those in non-border counties.
Slide 163
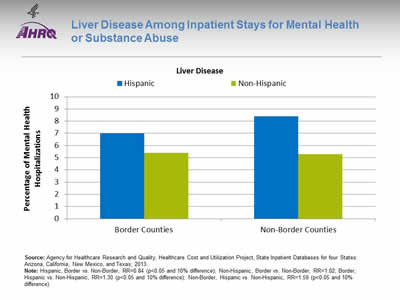
Liver Disease Among Inpatient Stays for Mental Health or Substance Abuse
Image: Bar chart shows percentage of mental health hospitalizations with liver disease. Border Counties: Hispanic - 7.0; Non-Hispanic - 5.4. Non-Border Counties: Hispanic - 8.4; Non-Hispanic - 5.3.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note: Hispanic, Border vs. Non-Border, RR=0.84 (p<0.05 and 10% difference); Non-Hispanic, Border vs. Non-Border, RR=1.02; Border, Hispanic vs. Non-Hispanic, RR=1.30 (p<0.05 and 10% difference); Non-Border, Hispanic vs. Non-Hispanic, RR=1.59 (p<0.05 and 10% difference).
- Compared with non-Hispanics, a higher percentage of Hispanics with an inpatient stay for mental health had liver disease, in both border and non-border counties.
- Among Hispanics, those in border counties were less likely to have liver disease than those in non-border counties.
Slide 164
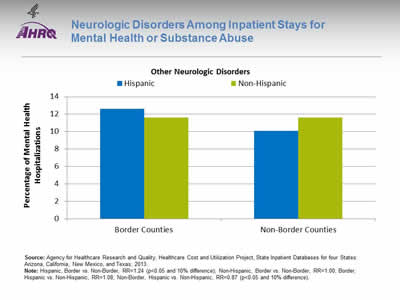
Neurologic Disorders Among Inpatient Stays for Mental Health or Substance Abuse
Image: Bar chart shows percentage of mental health hospitalizations with other neurologic disorders. Border Counties: Hispanic - 12.6; Non-Hispanic - 11.6. Non-Border Counties: Hispanic - 10.1; Non-Hispanic - 11.6.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note: Hispanic, Border vs. Non-Border, RR=1.24 (p<0.05 and 10% difference); Non-Hispanic, Border vs. Non-Border, RR=1.00; Border, Hispanic vs. Non-Hispanic, RR=1.08; Non-Border, Hispanic vs. Non-Hispanic, RR=0.87 (p<0.05 and 10% difference).
- A greater percentage of Hispanics in border counties with an inpatient stay for mental health had neurologic disorders, compared with Hispanics in non-border counties.
Slide 165
Hospital Care on the U.S.-Mexico Border
Border County Residents Treated at Non-Border Hospitals
Slide 166
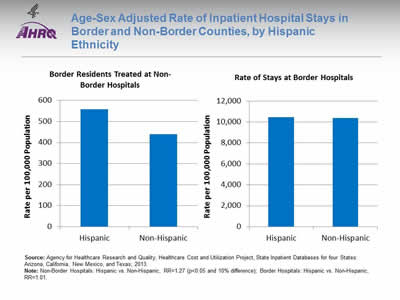
Age-Sex Adjusted Rate of Inpatient Hospital Stays in Border and Non-Border Counties, by Hispanic Ethnicity
Image: Bar charts show rate per 100,000 Population. Border Residents Treated at Non-Border Hospitals: Hispanic - 559, Non-Hispanic - 439. Rate of Stays at Border Hospitals: Hispanic - 10,459, Non-Hispanic - 10,381.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note: Non-Border Hospitals: Hispanic vs. Non-Hispanic, RR=1.27 (p<0.05 and 10% difference); Border Hospitals: Hispanic vs. Non-Hispanic, RR=1.01.
- By excluding border residents treated at non-border hospitals from the analyses above, we lost about 600 stays per 100,000 population.
- The rate of stays at border hospitals was similar for Hispanics and non-Hispanics. However, the rate of stays for border residents treated at non-border hospitals was 1.3 times as high for Hispanics as for non-Hispanics.
Slide 167
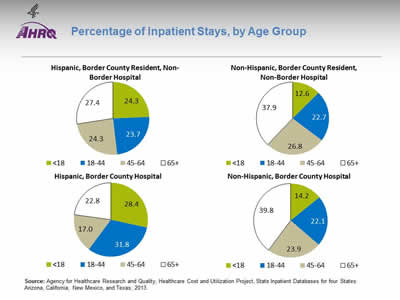
Percentage of Inpatient Stays, by Age Group
Image: Pie charts show percentage of Inpatient Stays, by Age Group. Hispanic, Border County Resident, Non-Border Hospital: Less than 18 - 24.3; 18-44 - 23.7; 45-64 - 24.3; 65 plus - 27.4. Hispanic, Border County Hospital: Less than 18 - 28.4; 18-44 - 31.8; 45-64 - 17.0; 65 plus - 22.8. Non-Hispanic, Border County Resident, Non-Border Hospital: Less than 18 - 12.6; 18-44 - 22.7; 45-64 - 26.8; 65 plus - 37.9. Non-Hispanic, Border County Hospital: Less than 18 - 14.2; 18-44 - 22.1; 45-64 - 23.9; 65 plus - 39.8.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note:
- The age distribution was generally similar for stays based on border county hospitals and border county residents treated at non-border hospitals.
Slide 168
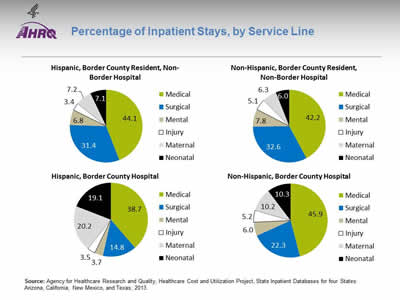
Percentage of Inpatient Stays, by Service Line
Image: Pie charts show percentage of Inpatient Stays, by Service Line. Hispanic, Border County Resident, Non-Border Hospital: Medical - 44.1; Surgical - 31.4; Mental - 6.8; Injury - 3.4; Maternal - 7.2; Neonatal - 7.1. Hispanic, Border County Hospital: Medical - 38.7; Surgical - 14.8; Mental - 3.7; Injury - 3.5; Maternal - 20.2; Neonatal - 19.1. Non-Hispanic, Border County Resident, Non-Border Hospital: Medical - 42.2; Surgical - 32.6; Mental - 7.8; Injury - 5.1; Maternal - 6.3; Neonatal - 6.0. Non-Hispanic, Border County Hospital: Medical - 45.9; Surgical - 22.3; Mental - 6.0; Injury - 5.2; Maternal - 10.2; Neonatal - 10.3.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013.
Note:
- Most discharges among border county residents treated at non-border hospitals were for surgical or medical reasons (75%) (versus, for instance, about 50% among Hispanics in border counties).
Slide 169
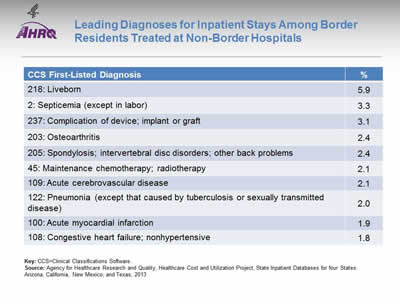
Leading Diagnoses for Inpatient Stays Among Border Residents Treated at Non-Border Hospitals
| Diagnosis | % |
|---|---|
| 218: Liveborn | 5.9 |
| 2: Septicemia (except in labor) | 3.3 |
| 237: Complication of device; implant or graft | 3.1 |
| 203: Osteoarthritis | 2.4 |
| 205: Spondylosis; intervertebral disc disorders; other back problems | 2.4 |
| 45: Maintenance chemotherapy; radiotherapy | 2.1 |
| 109: Acute cerebrovascular disease | 2.1 |
| 122: Pneumonia (except that caused by tuberculosis or sexually transmitted disease) | 2.0 |
| 100: Acute myocardial infarction | 1.9 |
| 108: Congestive heart failure; nonhypertensive | 1.8 |
Key: CCS=Clinical Classifications Software.
Source: Agency for Healthcare Research and Quality, Healthcare Cost and Utilization Project, State Inpatient Databases for four States: Arizona, California, New Mexico, and Texas; 2013
Slide 170
National Healthcare Quality and Disparities Report Chartbook on Health Care for Hispanics
Part 4: Health Care of Residents of the U.S.-Mexico Border
Summary
Slide 171
Key Findings
- Hospital data can be used to assess health care received by residents of the U.S.-Mexico border.
- Access to health care: Hispanics in border counties had the highest rates of uninsurance.
- Hispanics in border counties had higher hospitalization rates than Hispanics in non-border counties for:
- Diabetes.
- Injuries.
- Maternal and neonatal care.
- COPD.
- Chronic kidney disease.
- Obesity.
Slide 172
Key Findings
- When hospitalized for diabetes in border hospitals, Hispanics were more likely than non-Hispanics to experience:
- Amputation.
- Renal failure.
- Peripheral vascular disease.
- Paralysis.
- When hospitalized for mental health or substance abuse in border hospitals, Hispanics were more likely than non-Hispanics to have:
- Liver disease.
- Hispanics in border counties were more likely to be hospitalized in non-border hospitals than non-Hispanics.
Slide 173

National Healthcare Quality and Disparities Report Chartbook on Health Care for Hispanics
Part 4: Health Care of Residents of the U.S.-Mexico Border
Definitions
Slide 174
Conditions of Interest
- Cancers: Any Dx in CCS 24 (breast), 26 (cervix), 29 (prostate), or in range 140.x-149.x (oral).
- Cardiovascular: Any Dx in CCS 96-109.
- Diabetes: Any Dx in CCS 49-50:
- Lower-extremity amputation based on AHRQ PQI 16.
- HIV/AIDS: Any Dx in CCS 5.
- Maternal and Neonatal:
- Newborn: PDx in CCS 218 (normal) and CCS 219-224 (complicated):
- Neural tube defects: PDx in 756.17, 741.
- Delivery: PDx in CCS 196 (normal) and CCS 176-195 (complicated).
- Newborn: PDx in CCS 218 (normal) and CCS 219-224 (complicated):
- Mental Health and Substance Use: Any Dx in CCS 650-659, 662-670 (mental health) and CCS 660-661 (substance use).
- Environmental health: Any Dx in CCS 128 (asthma), 127 (COPD), 131 (respiratory failure), 122 and 132 (other respiratory including pneumonia).
- Injuries: Any external cause of injury code indicating motor vehicle accident and unintentional injuries (screen based on CDC classification for injuries).
- Obesity: Any Dx of 278.00, 278.01, and V778 by age (18+ adults; 0-17 children).
- Renal Failure: Any Dx in CCS 157 (acute) or CCS158 (chronic).
Key: Dx = diagnosis; CCS = Clinical Classifications Software; PQI = Prevention Quality Indicator; CDC = Centers for Disease Control and Prevention.
Slide 175
Service Line and Comorbidities
- Service line:
- Maternal: PDx in CCS 176-196.
- Neonatal: PDx in CCS 218-224.
- Mental Health: PDx in 650-670.
- Injury: PDX in range 800-990.4, 909.9, 910-994.9, and 995 (with some exclusions).
- Surgical: Surgical diagnosis-related group.
- Medical: All other discharges.
- Every discharge is assigned to one of the hospital service lines, based on the following hierarchical order: maternal and neonatal, mental health, injury, surgical, and medical.
- Comorbidities:
- AHRQ indicators for 29 comorbidities.
- Severity index is based on a weighted sum of the individual comorbidity indicators with more severe comorbidities having a higher weight. For example, the weight for metastatic cancer is 13 and the weight for chronic pulmonary disease is 3.