

Sensemaking and Learn From Defects for Perinatal Safety
AHRQ Safety Program for Perinatal Care
Slide 1: AHRQ Safety Program for Perinatal Care
Sensemaking and Learn From Defects for Perinatal Safety
Slide 2: Learning Objectives
Image: Four ascending steps show the learning objectives:
- Introduce CUSP and Sensemaking tools to identify defects or conditions.
- Discuss the relationship between CUSP and Sensemaking.
- Show how to apply CUSP and Sensemaking tools.
- Discuss how to share findings.
Slide 3: CUSP and Sensemaking Tools1
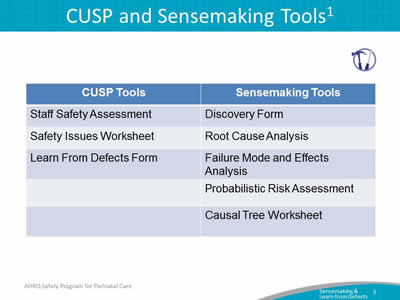
| CUSP Tools | Sensemaking Tools |
|---|---|
| Staff Safety Assessment | Discovery Form |
| Safety Issues Worksheet | Root Cause Analysis |
| Learn From Defects Form | Failure Mode and Effects Analysis |
| Probabilistic Risk Assessment | |
| Causal Tree Worksheet |
Slide 4: The Relationship Between CUSP and Sensemaking1,2,3
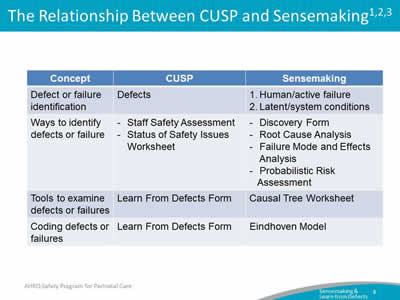
| Concept | CUSP | Sensemaking |
|---|---|---|
| Defect or failure identification | Defects |
|
| Ways to identify defects or failure |
|
|
| Tools to examine defects or failures | Learn From Defects Form | Causal Tree Worksheet |
| Coding defects or failures | Learn From Defects Form | Eindhoven Model |
Slide 5: Identify Defects Overview
- Define defects.
- Identify sources of defects.
- Apply CUSP tools to identify defects.
Slide 6: Sensemaking Overview4
- A conversation among members of an organization involved in an event/issue.
- The purpose is to reduce the ambiguity about the event/issue—literally to make sense of it.
- Each person brings their experience of that event/issue to the discussion.
- The conversation is the mechanism that combines that knowledge into a new, more understandable form for the members.
- Members develop a similar representation in their minds that allows for action that can be implemented and understood by all who participated in the conversation.
Slide 7: Examples of Defects or Failures That Affect Patient Safety
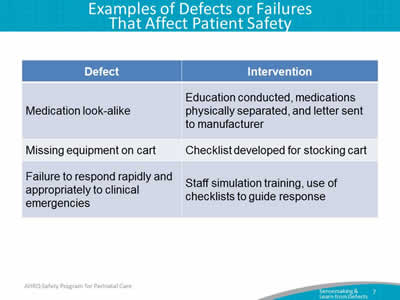
| Defect | Intervention |
|---|---|
| Medication look-alike | Education conducted, medications physically separated, and letter sent to manufacturer |
| Missing equipment on cart | Checklist developed for stocking cart |
| Failure to respond rapidly and appropriately to clinical emergencies | Staff simulation training, use of checklists to guide response |
Slide 8: Reason's Swiss Cheese Model5
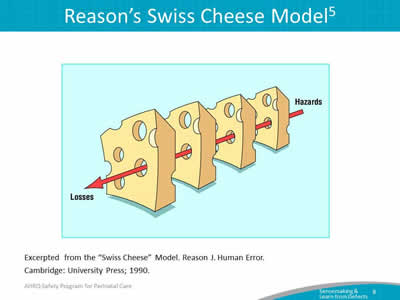
Image: Showing pieces of Swiss cheese, with a red arrow through matching holes in the cheese showing how Hazards become Losses.
Excerpted from the "Swiss Cheese" Model. Reason J. Human Error.
Cambridge: University Press; 1990.
Slide 9: Tools for Sensemaking and Learning From Defects
Tools for Sensemaking and Learning From Defects
Slide 10: Staff Safety Assessment
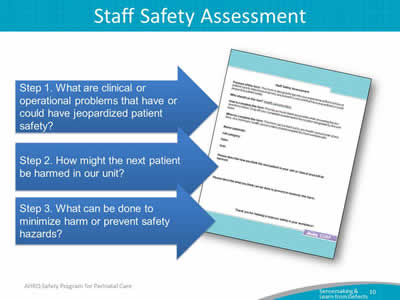
Image: Staff Safety Assessment Form. Use the Staff Safety Assessment Form to first, identify clinical or operational problems that have or could have negatively impacted patient safety. Second, describe how the next patient could be harmed. Then, lastly, describe what can be done to minimize patient harm or prevent this safety hazard.
Slide 11: Exercise
Please complete the following:
- List all defects that have the potential to cause to cause harm.
- Discuss the three greatest risks.
- Rank these factors.
Slide 12: Use the Safety Issues Worksheet for Senior Executive Partnership
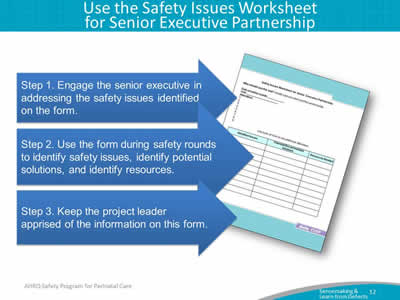
Image: Safety Issues Worksheet for Senior Executive Partnership. Use this form to engage the senior executive to address the safety issues identified in the form. Use this form during safety rounds, to identify safety issues, potential solutions, and available resources. Keep the project leader apprised of the information on this form.
Slide 13: Root Cause Analysis: Causal Tree Worksheet6
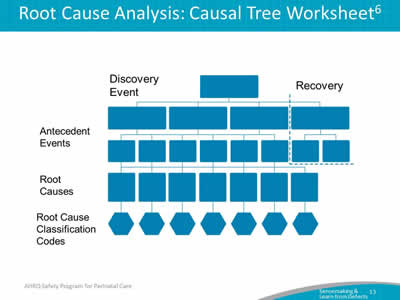
Image: The causal tree is made up of five rows. At the top of the tree and at the top row is the discovery event. The discovery event addresses what happened. The next two rows are labeled antecedent events and they ask a series of "whys" to understand the root cause of the event, which is the next row on the tree. The last row is the root cause classification codes which will be discussed later in this presentation. The left side of the tree is labeled the failure side, and a small part of the right side is labeled the recovery side. The recovery side is only completed if something prevented the event from reaching the patient.
Slide 14: Learning From Defects Overview
- Health care providers are adept at reacting to an event and finding a solution.
- Providers must also correct the factors that contribute to an event.
Slide 15: Exercise
Think of an unexpected situation that you recently encountered
- When did you know it was not what you expected?
- What were the clues?
- What sense did you make of it?
Slide 16: Learning From Defects: Four Questions
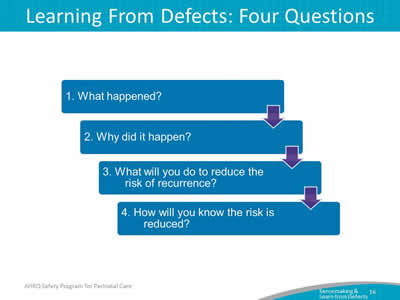
Image: Four text blocks list the Four Questions. Arrows pointing downward lead from one question to the next:
Question 1: What happened?
Question 2: Why did it happen?
Question 3: What will you do to reduce the risk of reoccurrence?
Question 4: How will you know it worked?
Slide 17: Causal Coding: Eindhoven Model6
- 20 separate event cause types in four categories:
- Technical.
- Organizational.
- Human.
- Other.
- Aim for three to seven root-cause codes for each event, a mixture of active and latent.
- All events involve multiple causes.
Slide 18: Summarize and Share Findings
- Create a one-page summary answering the four Learning From Defects questions.
- Share the summary within your organization
- Engage staff in face-to-face conversations to provide opportunities to learn from defects.
- Share de-identified information with others in your state collaborative (pending institutional approval).
Slide 19: Communicating the Learning

- Meeting to review data—monthly.
- Meeting with executive partner—monthly or more often.
- Executive review of data—monthly.
- Presentations to hospital colleagues as needed, including leadership, frontline staff, and hospital board.
Slide 20: Summary: Sensemaking and Learn From Defects
- Sensemaking and Learn From Defects share several common themes.
- Defects or failures are clinical or operational events that you do not want to happen again.
- CUSP and Sensemaking tools help teams identify defects and identify ways to deter them from occurring in the future.
Slide 21: References
- Battles JB, Kaplan HS, Van der Schaaf TW, et al. The attributes of medical event-reporting systems: Experience with a prototype medical event-reporting system for transfusion medicine. Arch Pathol Lab Med 1998 March;122:231-238. PMID: 9823860.
- Battles JB, Dixon NM, Borotkanics RJ, et al. Sensemaking of patient safety risks and hazards. Hlth Svcs Res 2006;41(Aug 4 Pt 2.):1555-75. PMID: 16898979.
- Sensemaking. Patient safety analysis training. [Columbia University's Digital Knowledge Ventures is no longer in operation.]
Slide 22: References
- Sensemaking. Patient safety analysis training. [Columbia University's Digital Knowledge Ventures is no longer in operation.]
- Pronovost PJ, Wu AW, and Sexton JB. Acute Decompensation after Removing a Central Line: Practical Approaches to Increasing Safety in the Intensive Care Unit. Ann Intern Med 2004 June;140(12):1025-33. PMID: 15197020.
- Sensemaking. Patient safety analysis training. [Columbia University's Digital Knowledge Ventures is no longer in operation.]
Slide 23: Disclaimers
Every effort was made to ensure the accuracy and completeness of this resource. However, the U.S. Department of Health and Human Services makes no warranties regarding errors or omissions and assumes no responsibility or liability for loss or damage resulting from the use of information contained within.
The U.S. Department of Health and Human Services cannot endorse, or appear to endorse derivate or excerpted materials, and it cannot be held liable for the content or use of adapted resources. Any adaptations of this resource must include a disclaimer to this effect.
Reference to any specific commercial products, process, service, manufacturer, company, or trademark does not constitute endorsement or recommendation by the U.S. Government, HHS, or AHRQ of the linked Web resources or the information, products, or services contained therein. The Agency does not exercise any control over the content on these sites.