

From February to March 2023, 1,113 physicians (76% private sector and 24% public sector) working in inpatient and outpatient settings participated in the survey. The survey’s average percent positive score across the three domains was 67.5 percent (the AHRQ score was 69%). Figure 1 shows the percent positive responses for each composite measure domain.
Figure 1. Percentage of positive responses from SBIBAE and AHRQ data from Survey on Patient Safety Culture Diagnostic Safety Supplemental Item Set for selected domains
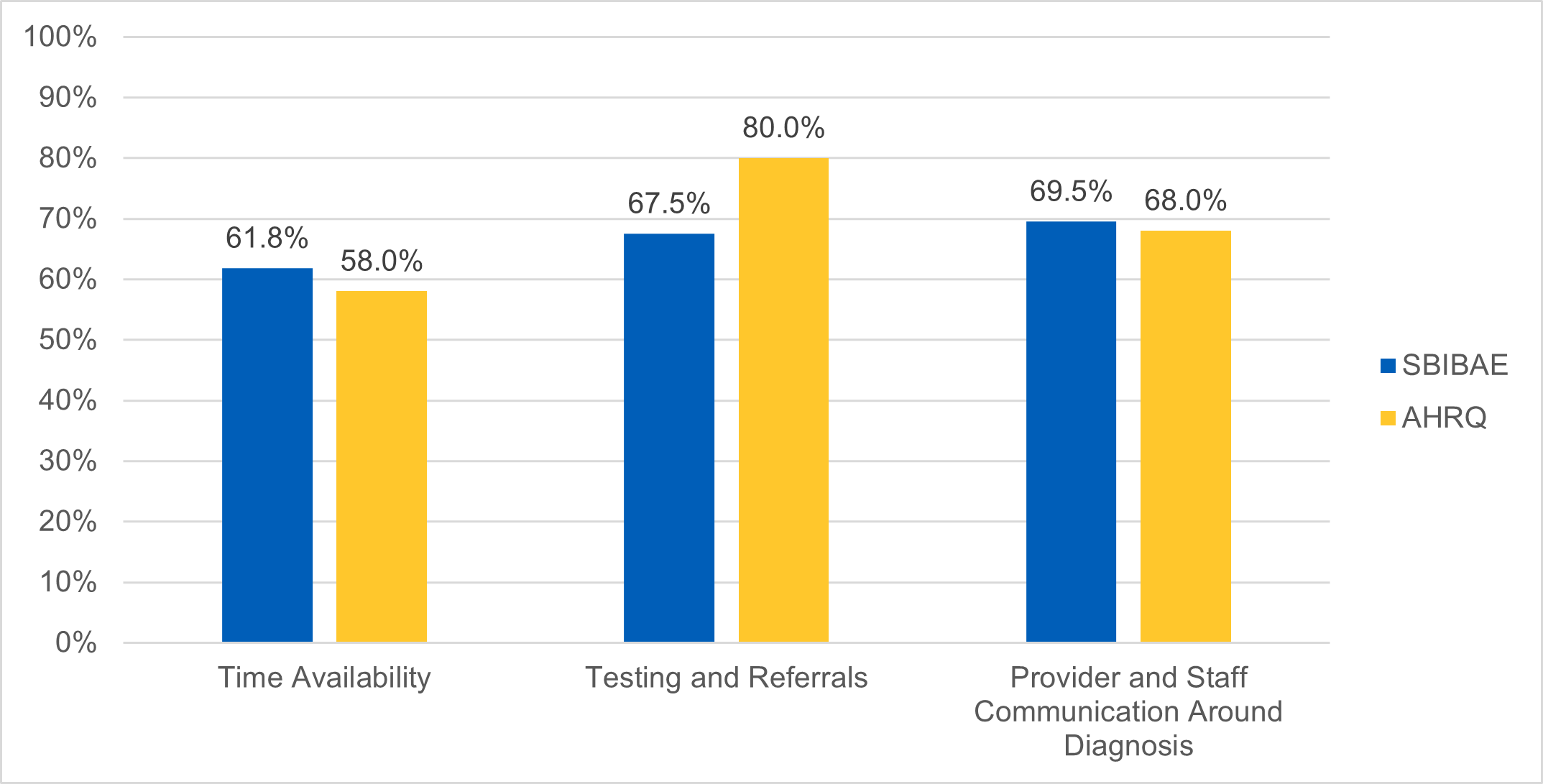
Key: SBIBAE = Sociedade Beneficente Israelita Brasileira Albert Einstein, São Paulo, Brazil).
Most physician respondents thought they had sufficient time to evaluate the patient during the consultation. But they thought other professionals, such as other members of a multidisciplinary care team (e.g., nurses, physiotherapists, nutritionists, pharmacists) did not have enough time to review the information relevant to the diagnosis (Table 1, items 1 and 2).
Survey findings revealed an excellent relationship with specialties that provided diagnostic support; more than 90 percent of physicians responded that they directly communicated with other specialists, radiologists, and pathologists when they needed clarification (Table 1, item 12). However, in the free-text comments on how to improve the diagnostic process, some comments reflected a large communication gap between the frontline physicians in the emergency department, intensive care unit professionals, and public sector radiologists.
Responses to the two feedback questions on failures in the diagnostic process suggested a gap in open communication regarding diagnostic errors. The first question related to whether a provider informs another provider in the office/system when they think that provider may have missed a diagnosis, and the second related to whether the office was informed when a missed, wrong, or delayed diagnosis happened in that office. These results were below the AHRQ average (Table 1, items 10 and 11) and revealed a significant gap within the institution in routinely providing specific feedback when a diagnosis is missed or incorrect, limiting learning opportunities for all care teams.
Table 1. Comparison of SBIBAE survey results and AHRQ SOPS Survey data
| Surveys on Patient Safety Culture® (SOPS®) Diagnostic Safety Item – Questions | SBIBAE* | AHRQ** |
|---|---|---|
| 1. The amount of time for appointments is long enough to fully evaluate the patient's presenting problem(s). | 88.7% | 63% |
| 2. Providers in this office have enough time to review the relevant information related to the patient’s presenting problem(s). | 40.4% | 64% |
| 3. Providers in this office finish their patient notes by the end of their regular workday. | 56.2% | 48% |
| 4. This office is effective at tracking a patient's test results from labs, imaging, and other diagnostic procedures. | 88.7% | 83% |
| 5. When this office doesn't receive a patient's test results, staff follow up. | 60.4% | 82% |
| 6. All test results are communicated to patients, even if the test results are normal. | 59.9% | 86% |
| 7. When this office makes a high priority referral, we try to confirm whether the patient went to the appointment. | 61.1% | 71% |
| 8. Providers in this office encourage staff to share their concerns about a patient's health condition. | 80.6% | 76% |
| 9. Providers document differential diagnoses when they have not ruled out other diagnoses. | 70.1% | 60% |
| 10. When a provider thinks another provider in this office/system may have missed a diagnosis, they inform that provider. | 54% | 55% |
| 11. When a missed, wrong, or delayed diagnosis happens in this office, we are informed about it. | 52.3% | 56% |
| 12. Providers in this office talk directly with specialists/radiologists/ pathologists when something needs clarification. | 90.6% | 87% |
*Sociedade Beneficente Israelita Brasileira Albert Einstein (SBIBAE).
**Agency for Healthcare and Quality (AHRQ), data from Survey on Patient Safety Culture Diagnostic Safety Supplemental Item Set.
Note: For each item, the percentages of positive responses were calculated by adding the strongly agree and agree responses and dividing by the total number of responses present, ignoring missing responses.