

Community-Acquired Pneumonia Clinical Decision Support Training: Primary Care Setting
Slide Presentation
Slide 1: Community-Acquired Pneumonia Clinical Decision Support Training
Primary Care Setting
Slide 2: Disclaimers and Acknowledgements
- This project was funded under contract/grant number HHSP233201500023I from the Agency for Healthcare Research and Quality (AHRQ), U.S. Department of Health and Human Services. The opinions expressed in this document are those of the authors and do not reflect the official position of AHRQ or the U.S. Department of Health and Human Services.
- The findings and conclusions in this document are those of the author(s), who are responsible for its content, and do not necessarily represent the views of AHRQ. No statement in this report should be construed as an official position of AHRQ or of the U.S. Department of Health and Human Services.
- This document is in the public domain and may be used and reprinted without permission except those copyrighted materials that are clearly noted in the document. Further reproduction of those copyrighted materials is prohibited without the specific permission of copyright holders. Note: "…under the Social Security Act [42 USC 1320b-10 (a)(2)(B)], reprinting or distribution of AHRQ or other HHS materials for a fee is prohibited without prior specific, written authorization."
Slide 3: Table of Contents
- Context:
- Background on Community-Acquired Pneumonia (CAP).
- Infectious Diseases Society of America/American Thoracic Society Guidelines on Management of CAP.
- Site of Care Decision.
- CURB-65 Criteria for 30-Day Mortality.
- Demonstration.
Slide 4: Background and Context

Background and Context
Slide 5: Community-Acquired Pneumonia
- Community-acquired pneumonia (CAP) is the 8th leading cause of death in the U.S.a
- 6 million cases of CAP reported annually.a
- High incidence among adults 65+.b
- CAP is among the top most commonly missed diagnoses.
a. FastStats: Pneumonia. Centers for Disease Control and Prevention. Centers for Disease Control and Prevention (CDC). http://www.cdc.gov/nchs/data/nvsr/nvsr64/nvsr64_02.pdf. Accessed January 10, 2017.
b. Stupka, J., Mortensen, E., Anzueto, A., et. al. Community-acquired pneumonia in elderly patients. Aging Health 2009;5 (6): 763-774. PMID: 21721597.
Slide 6: IDSA/ATS Consensus Guidelines on Management of CAP in Adults
- "Almost all of the major decisions regarding management of CAP, including diagnostic and treatment issues, revolve around the initial assessment of severity."c
- "The initial management decision after diagnosis is to determine the appropriate site of care."c
- Outpatient.
- Hospitalization on a medical unit.
- Admission to ICU.
c. Mandell, L., Wunderink, R., Anzueto, A., et. al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clinical Infectious Diseases 2007; 44, S27-S72. http://www.thoracic.org/statements/resources/mtpi/idsaats-cap.pdf.
Slide 7: Severity of Illness Scores
- "Can be used to identify patients with CAP who may be candidates for outpatient treatment."d
- Strong recommendation (most patients should receive this intervention).
- Level I evidence (high)—Evidence from well conducted, randomized controlled trials.
d. Mandell, L., Wunderink, R., Anzueto, A., et. al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clinical Infectious Diseases 2007; 44, S27-S72. http://www.thoracic.org/statements/resources/mtpi/idsaats-cap.pdf.
Slide 8: Site of Care
- "Cost of inpatient care of pneumonia is up to 25 times greater than outpatient care."e
- "Those treated in the outpatient setting are able to resume normal activity sooner."e
- "80% of patients prefer outpatient therapy."e
- "Hospitalization increases risk of thromboembolic events and superinfection by more virulent or resistant hospital bacteria."e
e. Mandell, L., Wunderink, R., Anzueto, A., et. al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clinical Infectious Diseases 2007; 44, S27-S72. http://www.thoracic.org/statements/resources/mtpi/idsaats-cap.pdf.
Slide 9: CURB-65 Criteria for 30-Day Mortality
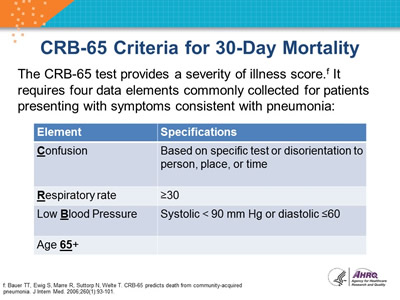
The CURB-65 test provides a severity of illness score.f It requires five data elements commonly collected for patients presenting with symptoms consistent with pneumonia:
| Element | Specifications |
|---|---|
| Confusion | Based on specific test or disorientation to person, place, or time |
| Respiratory rate | ≥30 |
| Low Blood Pressure | Systolic < 90 mm Hg or diastolic ≤60 |
| Age 65+ |
f. Mandell, L., Wunderink, R., Anzueto, A., et. al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clinical Infectious Diseases 2007; 44, S27-S72. http://www.thoracic.org/statements/resources/mtpi/idsaats-cap.pdf.
Slide 10: CURB-65 Scores Predict 30-Day Mortality
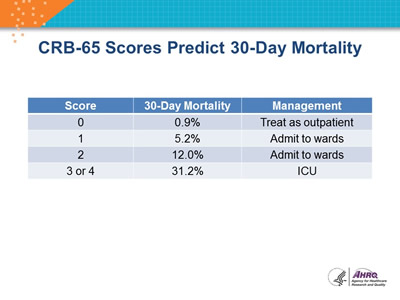
| Score | 30-Day Mortality | Management |
|---|---|---|
| 0 | 0.9% | Treat as outpatient |
| 1 | 5.2% | Admit to wards |
| 2 | 12.0% | Admit to wards |
| 3 or 4 | 31.2% | ICU |
Slide 11: CURB-65 CDS Tool
- Automatically extracts data from EHR (age, blood pressure, respiratory rate, and BUN when available) and calculates score.
- Provides option to add 1 to score if patient is found to be confused.
- Displays patient-specific 30-day mortality and guideline-recommended site of care.
- Records CURB-65 score in EHR and the clinician’s decision regarding disposition.
Slide 12: Important Notes from the IDSA/ATS Guideline
- "Objective criteria or scores should always be supplemented with physician determination of subjective factors, including the ability to safely and reliably take oral medication and the availability of outpatient support resources."i
- Strong recommendation.
- Level II evidence.
- "For patients with CURB-65 scores ≥2, more intensive treatment—i.e., hospitalization or, where appropriate and available, intensive in-home health care services—is usually warranted."i
- Moderate recommendation (Even if a majority would follow the recommended management, many practitioners may not).
- Level III evidence (evidence from case studies and expert opinion).
i. Mandell, L., Wunderink, R., Anzueto, A., et. al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clinical Infectious Diseases 2007; 44, S27-S72. http://www.thoracic.org/statements/resources/mtpi/idsaats-cap.pdf.
Slide 13: Demonstration
CAP CDS alert for the ED setting using CURB-65
Slide 14: Demonstration of the CAP CDS Alert Tool
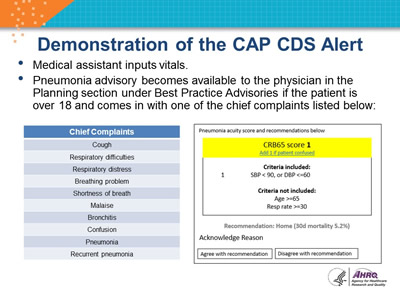
- After the chest x-ray is marked as "Complete" by the radiology technician, the pneumonia advisory will be triggered as an interruptive alert if the patient is over 18 and comes in with one of the chief complaints listed below:
| Chief Complaints |
| Cough |
| Respiratory difficulties |
| Respiratory distress |
| Breathing problem |
| Shortness of breath |
| Malaise |
| Bronchitis |
| Confusion |
| Pneumonia |
| Recurrent pneumonia |
Image: Sample CAP CDS Alert.
Slide 15: Demonstration of the CAP CDS Alert (cont.)
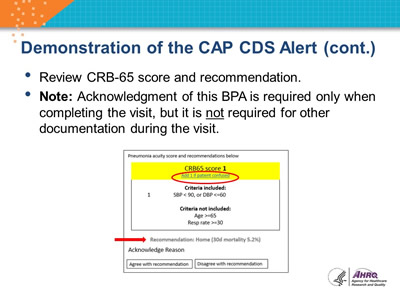
- Review CURB-65 score and recommendation.
- Note: Acknowledgment of this BPA is required only when completing the visit, but it is not required for other documentation during the visit.
Image: Sample CAP CDS Alert. The text 'Criteria included' is circled in red. A red arrow points to Recommendation: Home (30 d mortality 2.7%).
Slide 16: Demonstration of the CAP CDS Alert (cont.)
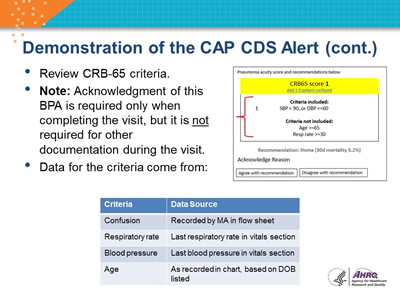
- Review CURB-65 criteria.
- Note: Acknowledgment of this BPA is required only when completing the visit, but it is not required for other documentation during the visit.
- Data for the criteria come from:
| Criteria | Data Source |
|---|---|
| Confusion | Recorded by MA in flow sheet |
| Respiratory rate | Last respiratory rate in vitals section |
| Blood pressure | Last blood pressure in vitals section |
| Age | As recorded in chart, based on DOB listed |
Image: Sample CAP CDS Alert. The sections for Criteria Included and Criteria not included are bracketed in red.
Slide 17: Demonstration of the CAP CDS Alert (cont.)
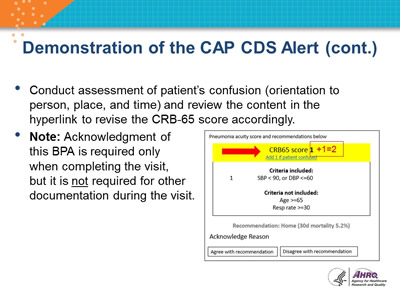
- Conduct assessment of patient’s confusion (orientation to person, place, and time) and review the content in the hyperlink to revise the CRB-65 score accordingly.
- Note: Acknowledgment of this BPA is required only when completing the visit, but it is not required for other documentation during the visit.
Image: Sample CAP CDS Alert. A red arrow points to the CRB65 score 1, and "1 plus 2" is added in red.
Slide 18: Demonstration of the CAP CDS Alert (cont.)
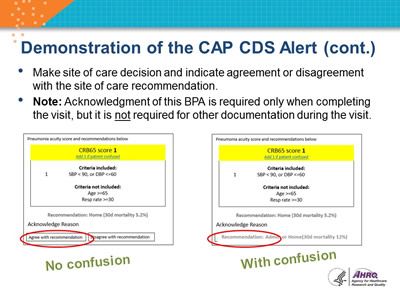
- Make site of care decision and indicate agreement or disagreement with the site of care recommendation.
- Note: Acknowledgment of this BPA is required only when completing the visit, but it is not required for other documentation during the visit.
Image: Two Sample CAP CDS Alerts. The "Agree with Recommendation" button is circled in red on the first one; this alert is captioned "No confusion." The text "Recommendation Admit" is circled in red on the second alert; this alert is captioned "With confusion."