

Early Mobility in the Intensive Care Unit: Slide Presentation
AHRQ Safety Program for Mechanically Ventilated Patients
Slide 1: AHRQ Safety Program for Mechanically Ventilated Patients
Early Mobility in the Intensive Care Unit
Slide 2: Learning Objectives
After this session, you will be able to—
- Apply outcomes from published research to support the benefits, safety, feasibility, and sustainability of an early mobility (EM) program in the intensive care unit (ICU).
Slide 3: Early ICU mobility therapy in the treatment of acute respiratory failure1
Design: Nonrandomized, controlled trial.
Subjects: 330 medical ICU (MICU) patients requiring ventilation on admission.
Interventions:
- Use of a mobility team:
- ICU registered nurse.
- ICU restorative nursing assistant.
- Physical therapy (PT).
- Implementing a rehabilitation protocol 7 days a week, starting within 48 hours of mechanical ventilation (MV).
1. Morris PE, Goad A, Thompson C, et al. Early intensive care unit mobility therapy in the treatment of acute respiratory failure. Crit Care Med 2008 Aug;36(8):2238-43. PMID: 18596631.
Slide 4: Main Outcomes1
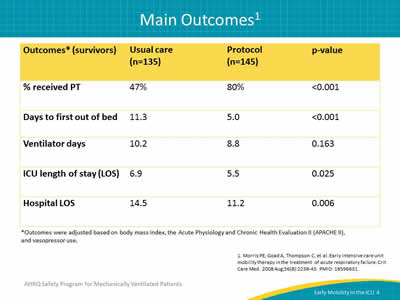
Image: Table showing main outcomes* from early ICU mobility therapy in the treatment of acute respiratory failure study.1
*Outcomes were adjusted based on body mass index, the Acute Physiology and Chronic Health Evaluation II (APACHE II), and vasopressor use.
1. Morris PE, Goad A, Thompson C, et al. Early intensive care unit mobility therapy in the treatment of acute respiratory failure. Crit Care Med 2008 Aug;36(8):2238-43. PMID: 18596631.
Slide 5: Conclusions1
- Mobility therapy delivered early in the course of acute respiratory failure was shown to be:
- Feasible.
- Safe.
- Cost effective.
- Associated with decreased ICU and hospital LOS.
1. Morris PE, Goad A, Thompson C, et al. Early intensive care unit mobility therapy in the treatment of acute respiratory failure. Crit Care Med 2008 Aug;36(8):2238-43. PMID: 18596631.
Slide 6: Early Physical and Occupational Therapy2
Design: Randomized controlled trial (RCT) at University of Chicago and University of Iowa.
Subjects: 104 MICU patients requiring MV.
Interventions: Physical therapy (PT) and occupational therapy (OT) starting at day 1-2 versus usual care (PT and OT starting at day 6-10).
2. Schweickert WD, Pohlman MC, Pohlman AS, et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomized controlled trial. Lancet 2009 May 30;373(9678):1874-82. PMID: 19446324.
Slide 7: Main Outcomes2
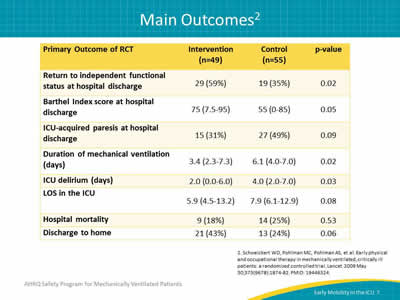
Image: Table showing main outcomes of an early physical and occupational therapy clinical trial.
2. Schweickert WD, Pohlman MC, Pohlman AS, et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomized controlled trial. Lancet 2009 May 30;373(9678):1874-82. PMID: 19446324.
Slide 8: How was PT/OT provided to get benefits?2
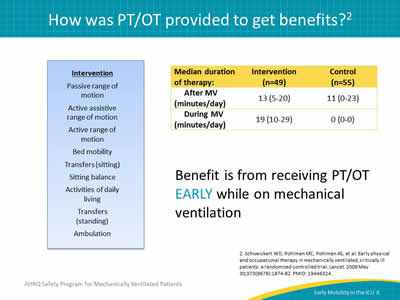
Benefit is from receiving PT/OT EARLY while on mechanical ventilation.
Intervention:
- Passive range of motion.
- Active assistive range of motion.
- Active range of motion.
- Bed mobility.
- Transfers (sitting).
- Sitting balance.
- Activities of daily living.
- Transfers (standing).
- Ambulation.
Images: Box indicating the interventions: passive range of motion, active assistive range of motion, active range of motion, bed mobility, transfers (sitting), sitting balance, activities of daily living, tranfers (standing), ambulation. Table showing the benefits of conducing EM therapies before versus after ventilation.
2. Schweickert WD, Pohlman MC, Pohlman AS, et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomized controlled trial. Lancet 2009 May 30;373(9678):1874-82. PMID: 19446324.
Slide 9: A Binational, Multicenter, Pilot, Feasibility, RCT of Early, Goal-Directed Mobilization in the ICU3
Design: Pilot RCT.
Subjects: 5 ICUs in Australia and New Zealand:
- 50 patients on mechanical ventilation for more than 24 hours.
Intervention: Protocolized early goal-directed mobility by PT:
- Seven days a week.
- Time to intervention, median (interquartile range [IQR]): 3 (2-4) days.
- Duration, median (IQR): 20 (0-40) vs. 7 (0-15) minutes per day, p=0.002.
3. Hodgson CL, Bailey M, Bellomo R, et al. TEAM Study Investigators. A binational multicenter pilot feasibility randomized controlled trial of early goal-directed mobilization in the ICU. Crit Care Med 2016 Jun;44(6):1145-52. PMID: 26968024.
Slide 10: Outcomes3
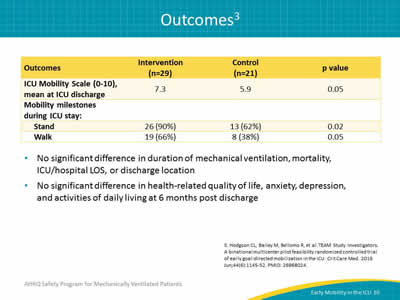
- No significant difference in duration of mechanical ventilation, mortality, ICU/hospital LOS, or discharge location.
- No significant difference in health-related quality of life, anxiety, depression, and activities of daily living at 6 months post discharge.
Image: Table shows Outcomes of a Binational, Multicenter, Pilot, Feasibility, RCT of Early, Goal-Directed Mobilization.
3. Hodgson CL, Bailey M, Bellomo R, et al. TEAM Study Investigators. A binational multicenter pilot feasibility randomized controlled trial of early goal-directed mobilization in the ICU. Crit Care Med 2016 Jun;44(6):1145-52. PMID: 26968024.
Slide 11: Safety3
- No serious adverse events.
- Events causing mobilization episode to stop:
- Intervention:
- Agitation (1).
- Control:
- Agitation (2).
- Transient hypotension (2).
- Intervention:
3. Hodgson CL, Bailey M, Bellomo R, et al. TEAM Study Investigators. A binational multicenter pilot feasibility randomized controlled trial of early goal-directed mobilization in the ICU. Crit Care Med 2016 Jun;44(6):1145-52. PMID: 26968024.
Slide 12: Early Activity is Feasible and Safe4
Design: Prospective cohort study.
Subjects: Eight-bed respiratory ICU in a community hospital:
- 103 patients.
Interventions: Activity events:
- Sit on bed.
- Sit on chair.
- Ambulate.
4. Bailey P, Thomsen GE, Spuhler VJ, et al. Early activity is feasible and safe in respiratory failure patients. Crit Care Med 2007 Jan;35(1):139-45. PMID: 17133183.
Slide 13: Activity Level on Last Day of Admission4
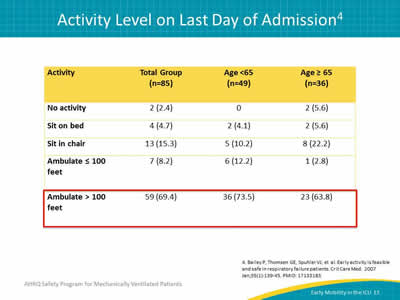
Image: Table showing the activity level on the last day of admission for patients in the ICU. A majority of patients, both over and under 65 years of age, were able to ambulate >100 feet.
4. Bailey P, Thomsen GE, Spuhler VJ, et al. Early activity is feasible and safe in respiratory failure patients. Crit Care Med 2007 Jan;35(1):139-45. PMID: 17133183.
Slide 14: Adverse Events4
- 9 patients had 14 adverse event (<1% of activities):
- Falls to knees without injury (5).
- Systolic blood pressure <90 mmHg (4).
- Oxygen saturation <80% (3).
- Nasal feeding tube removal (1).
- Systolic blood pressure >200 mmHg (1).
- No extubations.
- No patients required added therapy or increased LOS.
- No extra cost was incurred.
4. Bailey P, Thomsen GE, Spuhler VJ, et al. Early activity is feasible and safe in respiratory failure patients. Crit Care Med 2007 Jan;35(1):139-45. PMID: 17133183.
Slide 15: Safety of Physical Therapy Interventions5
Design: Prospective observational study, data collected June 2009–December 2011.
Subjects: Academic medical center MICU:
- 1,110 admissions with at least one PT session.
Intervention: Routine physical therapy:
- 5,267 total PT treatments (not individual activities).
- 66% of PT days: sitting at edge of bed or higher level.
5. Sricharoenchai T, Parker AM, Zanni JM, et al. Safety of physical therapy interventions in critically ill patients: a single-center prospective evaluation of 1110 intensive care unit admissions. J Crit Care 2014 Jun;29(3):395-400. PMID: 24508202.
Slide 16: Safety of Physical Therapy Interventions5
34 potential safety events in 25 of 1,110 admissions.
- 0.6% of PT sessions (i.e., 6 per 1,000 PT treatment):
- 80% of events were transient physiological (heart rate, blood pressure, blood oxygen level).
- 4 events required any treatment (8 per 10,000 PT treatment):
- Dislodgement of orogastric tube (2).
- Dislodgement of arterial line (1).
- Fall with laceration and suture (1).
5. Sricharoenchai T, Parker AM, Zanni JM, et al. Safety of physical therapy interventions in critically ill patients: a single-center prospective evaluation of 1110 intensive care unit admissions. J Crit Care 2014 Jun;29(3):395-400. PMID: 24508202.
Slide 17: Early Mobility in a Trauma and Burns ICU6
Design: Retrospective cohort study at an academic medical center.
Subjects: 2,176 trauma and burn ICU patients,
- Pre (n=1044) and post (n=1132) EM program.
- Not limited to patients on MV.
Intervention: PT consult at admission combined with RN/PT progressive mobility program versus usual care.
6. Clark DE, Lowman JD, Griffin RL, et al. Effectiveness of an early mobilization protocol in a trauma and burns intensive care unit: a retrospective cohort study. Phys Ther 2013 Feb;93(2):186-96. PMID: 22879442.
Slide 18: Complications to ICU Stay6
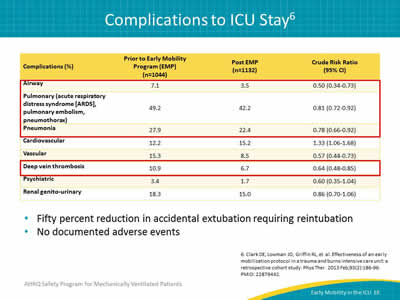
Image: Table showing percent of different complications occurring during an ICU stay.
- Fifty percent reduction in accidental extubation requiring reintubation.
- No documented adverse events.
6. Clark DE, Lowman JD, Griffin RL, et al. Effectiveness of an early mobilization protocol in a trauma and burns intensive care unit: a retrospective cohort study. Phys Ther 2013 Feb;93(2):186-96. PMID: 22879442.
Slide 19: Barriers6
- Staff concerns prior to implementation:
- Time.
- Safety.
- Used previously published literature.
- Time was an issue at the beginning.
- No longer an issue as staff became more accustomed to practice.
6. Clark DE, Lowman JD, Griffin RL, et al. Effectiveness of an early mobilization protocol in a trauma and burns intensive care unit: a retrospective cohort study. Phys Ther 2013 Feb;93(2):186-96. PMID: 22879442.
Slide 20: Barriers to Activity in the ICU7
- Time requirements and adequate staffing.
- Need for staff training.
- Need for team work and coordination.
- Oversedation of ICU patients.
- Dislodgement of devices (central venous catheter, endotracheal tube, feeding tubes).
- Worsening gas exchange.
- Unstable hemodynamics.
- Inadequate patient comfort, pain control.
7. Zanni JM, Korupolu R, Fan E, et al. Rehabilitation therapy and outcomes in acute respiratory failure: an observational pilot project. J Crit Care 2010 Jun;25(2):254-62. PMID: 19942399.
Slide 21: 5-Year Sustainability of Time to Physical Therapy8
Design: Pre/post evaluation:
- Pre-quality improvement (QI) (2004–2007) versus post-QI (2009–2012).
Subjects: 243 consecutive patients with ARDS.
Objectives:
- Evaluate the sustainability of MICU early rehab QI over 5 years.
- Evaluate factors with timing of onset of active PT.
8. Dinglas VD, Parker AM, Reddy DR, et al. A quality improvement project sustainably decreased time to onset of active physical therapy intervention in patients with acute lung injury. Ann Am Thorac Soc 2014 Oct;11(8):1230-8. PMID: 25167767.
Slide 22: Pre- Versus Post-Implementation8
- Receipt of physical therapy – 24% vs. 89%, p<0.001.
- Able to stand, transfer, or ambulate – 7% vs. 64%, p=<0.001.
8. Dinglas VD, Parker AM, Reddy DR, et al. A quality improvement project sustainably decreased time to onset of active physical therapy intervention in patients with acute lung injury. Ann Am Thorac Soc 2014 Oct;11(8):1230-8. PMID: 25167767.
Slide 23: 5-Year Sustainability of Time to PT Postacute Lung Injury Diagnosis8
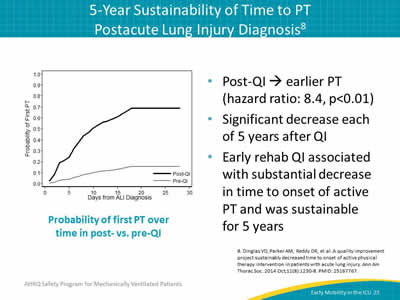
- Post-QI → earlier PT (hazard ratio: 8.4, p<0.01).
- Significant decrease each of 5 years after QI.
- Early rehab QI associated with substantial decrease in time to onset of active PT and was sustainable for 5 years.
Image: Graph showing the probability of first PT over time post vs. pre QI.
8. Dinglas VD, Parker AM, Reddy DR, et al. A quality improvement project sustainably decreased time to onset of active physical therapy intervention in patients with acute lung injury. Ann Am Thorac Soc 2014 Oct;11(8):1230-8. PMID: 25167767.
Slide 24: Conclusions
Conclusions
Slide 25: Conclusions—Benefits
- Decreased ICU and hospital length of stay.1,2
- Decreased duration of mechanical ventilation and days with delirium.2
- Increased return to independent functional status at hospital discharge.2
1. Morris PE, Goad A, Thompson C, et al. Early intensive care unit mobility therapy in the treatment of acute respiratory failure. Crit Care Med 2008 Aug;36(8):2238-43. PMID: 18596631.
2. Schweickert WD, Pohlman MC, Pohlman AS, et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomized controlled trial. Lancet 2009 May 30;373(9678):1874-82. PMID: 19446324.
Slide 26: Conclusions—Safety
- Adverse events ranged from agitation to transient physiological events to dislodgements and to falls (none of the falls were considered serious).
- Adverse events ranged from 2.3 to 8.7 per 100 patients.3-5
3. Hodgson CL, Bailey M, Bellomo R, et al. TEAM Study Investigators. A binational multicenter pilot feasibility randomized controlled trial of early goal-directed mobilization in the ICU. Crit Care Med 2016 Jun;44(6):1145-52. PMID: 26968024.
4. Bailey P, Thomsen GE, Spuhler VJ, et al. Early activity is feasible and safe in respiratory failure patients. Crit Care Med 2007 Jan;35(1):139-45. PMID: 17133183.
5. Sricharoenchai T, Parker AM, Zanni JM, et al. Safety of physical therapy interventions in critically ill patients: a single-center prospective evaluation of 1110 intensive care unit admissions. J Crit Care 2014 Jun;29(3):395-400. PMID: 24508202.
Slide 27: Conclusions—Feasiblity
- There are significant barriers to overcome.6,7
- However, the authors of all studies were in agreement that their early mobility program was feasible and it is a benefit to the patient.
6. Clark DE, Lowman JD, Griffin RL, et al. Effectiveness of an early mobilization protocol in a trauma and burns intensive care unit: a retrospective cohort study. Phys Ther 2013 Feb;93(2):186-96. PMID: 22879442.
7. Zanni JM, Korupolu R, Fan E, et al. Rehabilitation therapy and outcomes in acute respiratory failure: an observational pilot project. J Crit Care 2010 Jun;25(2):254-62. PMID: 19942399.
Slide 28: Conclusions—Sustainability
- Dinglas et al. were able to show a 5-year sustainability in their early mobility program.8
- Clark et al. plan to sustain their improvements by hiring more physical therapists to assure their success.6
8. Dinglas VD, Parker AM, Reddy DR, et al. A quality improvement project sustainably decreased time to onset of active physical therapy intervention in patients with acute lung injury. Ann Am Thorac Soc 2014 Oct;11(8):1230-8. PMID: 25167767.
Slide 29: References
1. Morris PE, Goad A, Thompson C, et al. Early intensive care unit mobility therapy in the treatment of acute respiratory failure. Crit Care Med 2008 Aug;36(8):2238-43. PMID: 18596631.
2. Schweickert WD, Pohlman MC, Pohlman AS, et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomized controlled trial. Lancet 2009 May 30;373(9678):1874-82. PMID: 19446324.
3. Hodgson CL, Bailey M, Bellomo R, et al. TEAM Study Investigators. A binational multicenter pilot feasibility randomized controlled trial of early goal-directed mobilization in the ICU. Crit Care Med 2016 Jun;44(6):1145-52. PMID: 26968024.
4. Bailey P, Thomsen GE, Spuhler VJ, et al. Early activity is feasible and safe in respiratory failure patients. Crit Care Med 2007 Jan;35(1):139-45. PMID: 17133183.
Slide 30: References
5. Sricharoenchai T, Parker AM, Zanni JM, et al. Safety of physical therapy interventions in critically ill patients: a single-center prospective evaluation of 1110 intensive care unit admissions. J Crit Care 2014 Jun;29(3):395-400. PMID: 24508202.
6. Clark DE, Lowman JD, Griffin RL, et al. Effectiveness of an early mobilization protocol in a trauma and burns intensive care unit: a retrospective cohort study. Phys Ther 2013 Feb;93(2):186-96. PMID: 22879442.
7. Zanni JM, Korupolu R, Fan E, et al. Rehabilitation therapy and outcomes in acute respiratory failure: an observational pilot project. J Crit Care 2010 Jun;25(2):254-62. PMID: 19942399.
8. Dinglas VD, Parker AM, Reddy DR, et al. A quality improvement project sustainably decreased time to onset of active physical therapy intervention in patients with acute lung injury. Ann Am Thorac Soc 2014 Oct;11(8):1230-8. PMID: 25167767.