

Assess and Adapt: Understanding the Science of Safety and Reliability
Slide Presentation
Slide 1
Assess and Adapt: Understanding the Science of Safety and Reliability
Lisa H. Lubomski, PhD
Assistant Professor, Johns Hopkins Medicine
Armstrong Institute for Patient Safety & Quality
Department of Anesthesiology & Critical Care Medicine
Image: Photo of Dr. Lubomski on bottom left, and On the CUSP logo on bottom right.
Slide 2
Learning Objectives
- Define the need for creating reliability in health care
- Describe “CUSP” as an intervention to improve reliability of health care delivery and outcomes
- Discuss the why and how of CUSP Step One: Understanding the Science of Safety
Slide 3
How Dangerous is Health Care?
- Fewer than one death per 100,000 encounters
- Nuclear power
- European railroads
- Scheduled airlines
- One death in less than 100,000 but more than 1,000 encounters
- Driving
- Chemical manufacturing
- More than one death per 1,000 encounters
- Bungee jumping
- Mountain climbing
- Health care
Slide 4
Putting Safety in Context
- Advances in medicine have led to positive outcomes:
- Most childhood cancers are curable
- AIDS is now a chronic disease
- Life expectancy has increased 10 years since the 1950s
- However, sponges are still found inside patients’ bodies after operations.
Image: Cartoon image of health professionals looking at an x-ray image.
Slide 5
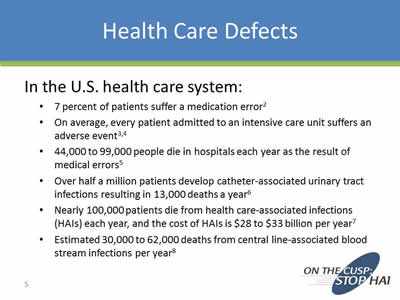
Health Care Defects
- 7 percent of patients suffer a medication error2
- On average, every patient admitted to an intensive care unit suffers an adverse event3, 4
- 44,000 to 99,000 people die in hospitals each year as the result of medical errors5
- Over half a million patients develop catheter-associated urinary tract infections resulting in 13,000 deaths a year6
- Nearly 100,000 patients die from health care-associated infections (HAIs) each year, and the cost of HAIs is $28 to $33 billion per year7
- Estimated 30,000 to 62,000 deaths from central line-associated blood stream infections per year8
Slide 6
Challenging… So Many Solutions?
Montage of images of different safety tool logos including CUSP, TeamSTEPPS, Model for Improvement, LEAN, and Baldridge Criteria for Improvement.
Slide 7

The Need to Improve Safety Culture is Not Unique to Health Care
Image: The front page of the Baltimore Sun newspaper from 2003, with the headline "NASA's safety culture blamed" circled in red.
Slide 8
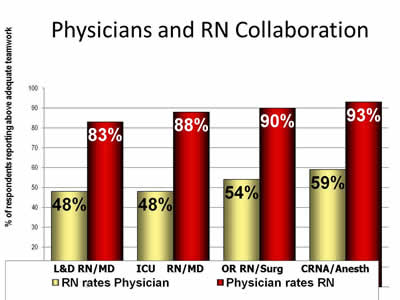
Physicians and RN Collaboration
Image: Bar chart showing rates of collaboration between Labor & Delivery nurses and doctors, intensive care unit nurses and doctors, operating room nurses and surgeons, and certified registered nurse assistants and doctors. On average, doctors rated teamwork twice as high as nurses or other health professionals.
Slide 9
Goals of CAUTI Project
- To reduce average CAUTI rates in participating unit by 25% through the following steps:
- To educate health care workers about the appropriate management of urinary catheters, including indications for the placement and continued use of urinary catheters
- To prevent the placement of unnecessary urinary catheters
- To promptly remove urinary catheters that are no longer needed
Slide 10
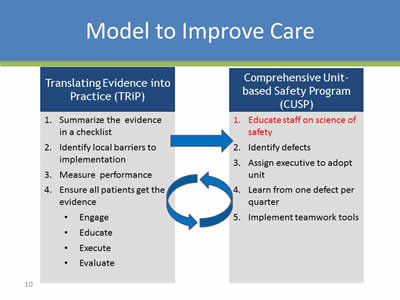
Model to Improve Care
Translating Evidence Into Practice (TRIP)
- Summarize the evidence in a checklist
- Identify local barriers to implementation\
- Measure performance
- Ensure all patients get the evidence
- Engage
- Educate
- Execute
- Evaluate
Lead to:
Comprehensive Unit-based Safety Program (CUSP)
- Educate staff on science of safety
- Identify defects
- Assign executive to adopt unit
- Learn from one defect per quarter
- Implement teamwork tools\
Slide 11
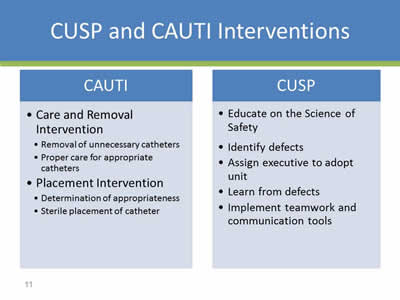
CUSP and CAUTI Interventions
CAUTI
- Care and Removal Intervention
- Removal of unnecessary catheters
- Proper care for appropriate catheters\
- Placement Intervention
- Determination of appropriateness
- Sterile placement of catheter
CUSP
- Educate on the Science of Safety
- Identify defects
- Assign executive to adopt unit
- Learn from defects
- Implement teamwork and communication tools
Slide 12
What is CUSP?
- Comprehensive Unit-based Safety Program
- An intervention to improve teamwork and safety culture and learn from mistakes
- http://www.ahrq.gov/professionals/education/curriculum-tools/cusptoolkit/index.html
Slide 13
Use of CUSP Results In:
- Improved engagement of staff and senior leadership
- Improved communication among care team members
- Shared mental models
- Knowledge and awareness of potential hazards and barriers to safety
- Collaborative focus on systems of care
Slide 14

CUSP Toolkit
Image: CUSP logo with the Understand the Science of Safety section enlarged.
Slide 15
The Science of Safety
- Every system is perfectly designed to achieve its end results
- Safe design principles must be applied to technical work and teamwork
- Teams make wise decisions when there is diverse and independent input
Slide 16
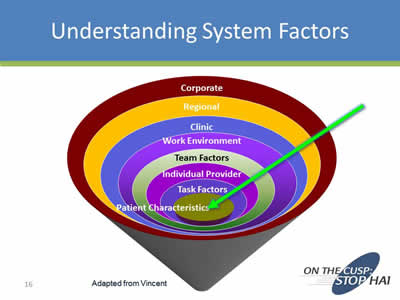
Understanding System Factors
Image: Cone-shaped graphic with concentric rings. Rings from inner to outer are: Patient Characteristic, Task Factors, Individual Provider, Team Factors, Work Environment, Clinic, Regional, and Corporate.
Slide 17
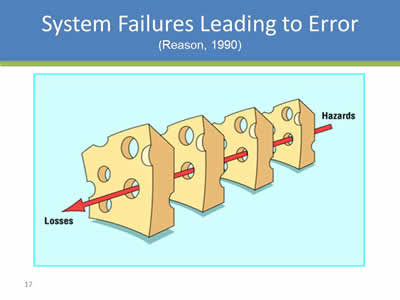
System Failures Leading to Error
(Reason, 1990)
Image: Four chunks of swiss cheese with a red arrow going through one of the holes with Hazards at the end of the last chunk leading to Losses at the first chunk.
Slide 18
Three Principles of Safe Design
- Standardize
- Create independent checks
- Learn when things go wrong
Slide 19

Eliminate Steps
Image: A bank ATM machine.
Slide 20

Standardize
Image: Health professional in a surgical gown and mask posing next to an equipment cart and in front a poster explaining CAUTI prevention procedures.
Slide 21

Create Independent Checks
Slide 22
Evidence-based Behaviors to Prevent CLABSI
(MMWR. 2002;51:RR-10)
- Remove Unnecessary Lines
- Wash Hands Prior to Procedure
- Use Maximal Barrier Precautions
- Clean Skin with Chlorhexidine
- Avoid Femoral Lines
Slide 23
Independent Check: CLABSI Insertion Checklist
(Crit Care Med 2004;32(10):2014.)
- Before the procedure, did clinician inserting line:
- Wash hands
- Sterilize procedure site
- Drape entire patient in a sterile fashion
- During the procedure, did they:
- Use sterile gloves, mask and sterile gown
- Maintain a sterile field
- Did all personnel assisting with procedure follow the above precautions?
- Are staff empowered to stop the procedure if violation occurs?
Slide 24
Learn When Things Go Wrong
- First vs. Second order problem solving
- Fixing the immediate problem
- Fixing the system factors that allowed the problem to occur
Slide 25
Principles of Safe Design Apply to Technical and Teamwork
Slide 26
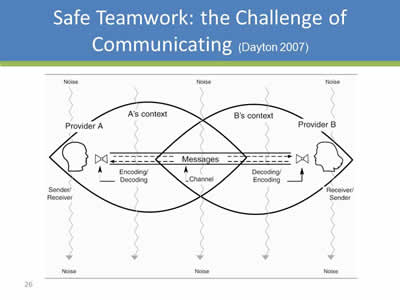
Safe Teamwork: the Challenge of Communicating
(Dayton 2007)
Image: Diagram showing the challenges of encoding and decoding messages between two persons.
Slide 27
Teams Make Wise Decisions When There is Diverse and Independent Input
(Heifetz R, 1994)
- Wisdom of Crowds*
- Seek involvement from clinicians at all levels of the organization
- Alternate between convergent and divergent thinking:
- What does everyone think?
- What will be “our” policy/procedure/practice?
- Get from the dance floor to the balcony level
- Individual challenges
- System challenges
Slide 28
Science of Safety Education
- Mandatory Science of Safety Training
- Adaptive Activity/training done Prior to CAUTI technical work
- Safety Survey to identify at-risk Departments
- Unit Safety Teams
- Unit Safety Action Plans
- Senior Executive Partnerships
Slide 29
Learning from CUSP
- Culture is local:
- Implement in a few units, adapt and spread
- Include frontline staff on improvement team
- Not linear process:
- Iterative cycles
- Takes time to improve culture
- Couple with clinical focus:
- No success improving culture alone
- CUSP alone viewed as ‘soft’
- Vehicle for clinical change
Slide 30
Principles: Science of Safety
- Accept that we will make mistakes
- Focus on systems rather than blame
- Speak up if you have concerns listen when others do
- Create clear goals, ask questions early
- Standardize, create independent checks, and learn from mistakes
Slide 31
Summary
- Safety is a property of system
- We need lenses to see the system
- We need to provide a safe space to voice what we see
- CUSP is a structured approach to learn from mistakes and improve safety culture
- Educating on the Science of Safety is Step 1
Slide 32
Summary
- Every system is designed to achieve its anticipated results
- The principles of safe design are standardize when you can, create independent checks, and learn from defects
- The principles of safe design apply to technical work and teamwork
- Teams make wise decisions when there is diverse input
Slide 33
Action Items
- Have all members of the CUSP CAUTI Team view the Science of Improving Patient Safety video
- Put together a roster of who on your unit needs to view the Science of Safety video
- Develop a plan to have all staff on your unit view the Science of Improving Patient Safety video
- Assess what technologies you have available for staff to view
- Identify times for viewing it (e.g., staff meetings, individual admin hours)
Slide 34
References
- Agency for Healthcare Research and Quality, Department of Defense. TeamSTEPPS. Available at www.ahrq.gov/teamsteppstools/instructor/index.html
- Bates DW, Cullen DJ, Laird N, et al. Incidence of adverse drug events and potential adverse drug events. JAMA. 1995;274(1):29–34.
- Donchin Y, Gopher D, Olin M, et al. A look into the nature and causes of human errors in the intensive care unit. Crit Care Med. 1995;23:294–300.
- Andrews LB, Stocking C, Krizek T, et al. An alternative strategy for studying adverse events in medical care. Lancet. 349:309–313,1997.
Slide 35
References
- Kohn L, Corrigan J, Donaldson M. To err is human: building a safer health system. Washington, DC: National Academy Press; 1999.
- Scott, RD. The Direct Medical Costs of Healthcare-Associated Infections in U.S. Hospitals and the Benefits of Prevention. March 2009. http://www.cdc.gov/ncidod/dhqp/pdf/Scott_CostPaper.pdf
- Klevens M, Edwards J, Richards C, et al. Estimating Health Care-Associated Infections and Deaths in U.S. Hospitals, 2002. PHR. 2007;122:160–166.
- Ending health care-associated infections, AHRQ, Rockville, MD; 2009. http://www.ahrq.gov/research/findings/factsheets/errors-safety/haicusp/index.html.
- Vincent C, Taylor-Adams S, Stanhope N. Framework for analysing risk and safety in clinical medicine. BMJ. 1998;316:1154–57
Slide 36
References
- Reason JT. Human Error. New York, NY: Cambridge University Press, 1990.
- Heifetz R. Leadership without easy answers, president and fellows of Harvard College. Cambridge, MA: Harvard University Press;1994.
- Dayton E, Henriksen K. Communication failure: basic components, contributing factors, and the call for structure. Jt Comm J Qual Patient Saf. 2007;33(1): 34–47.
- Pronovost P, Needham D, Berenholtz S, et al. An intervention to decrease catheter-related bloodstream infections in the ICU. New Engl J Med. 2006;355(26):2725–32.
Slide 37
Thank you!
Questions?
Slide 38
Funding
Prepared by the Health Research & Educational Trust of the American Hospital Association with contract funding provided by the Agency for Healthcare Research and Quality through the contract, “National Implementation of Comprehensive Unit-based Safety Program (CUSP) to Reduce Catheter-Associated Urinary Tract Infection (CAUTI), project number HHSA290201000025I/HHSA29032001T, Task Order #1.”