

Patient and Family-Centered Care
Slide Presentation
Slide 1
Patient and Family-Centered Care
Christine Goeschel ScD, MPA, MPS, RN, FAAN
Assistant Professor, Johns Hopkins School of Medicine
Joint Appointment, Schools of Public Health and Nursing
And
Gail Panoff
Chair, Patient and Community Engagement Council
St. Joseph Mercy Health System Ann Arbor, MI
Slide 2
Learning Objectives
- Describe CUSP as an intervention to improve health care delivery and care outcomes
- Define patient-and-family engagement
- Discuss ways that CUSP can be used to support patient and family engagement
- State how one patient and family experience council engages patients and their families in care outcomes at the hospital
Slide 3
Patient and Family Engagement and CUSP CAUTI
More work, Different work, Same work?
Presented by:
Chris Goeschel, ScD MPA MPS RN FAAN
Slide 4
Challenging …So Many Solutions?
Images: Logos and screen shots from the Toyota Lean Manufacturing Program, Baldridge, TeamSTEPPS, PDSA, with the CUSP logo in the center.
Slide 5
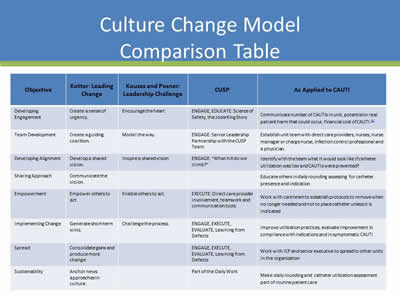
Culture Change Model Comparison Table
| Objective | Kotter: Leading Change | Kouzes and Posner: Leadership Challenge | CUSP | As Applied to CAUTI |
|---|---|---|---|---|
| Developing Engagement | Create a sense of urgency. | Encourage the heart. | ENGAGE, EDUCATE: Science of Safety, the Josie King Story | Communicate number of CAUTIs in unit, potential or real patient harm that could occur, financial cost of CAUTI.1 |
| Team Development | Create a guiding coalition. | Model the way. | ENGAGE: Senior Leadership Partnership with the CUSP Team | Establish unit team with direct care providers, nurses, nurse manager or charge nurse, infection control professional and a physician. |
| Developing Alignment | Develop a shared vision. | Inspire a shared vision. | ENGAGE: “What hill do we climb?” | Identify with the team what it would look like if catheter utilization was low and CAUTIs were prevented? |
| Sharing Approach | Communicate the vision. | Educate others in daily rounding assessing for catheter presence and indication | ||
| Empowerment | Empower others to act | Enable others to act. | EXECUTE: Direct care provider involvement, teamwork and communication tools | Work with care team to establish protocols to remove when no longer needed and not to place catheter unless it is indicated |
| Implementing Change | Generate short-term wins. | Challenge the process. | ENGAGE, EXECUTE, EVALUATE, Learning from Defects | Improve utilization practices, evaluate improvement in compliance with indications and in symptomatic CAUTI |
| Spread | Consolidate gains and produce more change | ENGAGE, EXECUTE, EVALUATE, Learning from Defects | Work with ICP and senior executive to spread to other units in the organization | |
| Sustainability | Anchor news approaches in culture. | Part of the Daily Work | Make daily rounding and catheter utilization assessment part of routine patient care |
Slide 6
What is CUSP?
- Comprehensive Unit-based Safety Program
- An intervention to learn from mistakes and improve safety culture for sustained improved patient outcomes
Slide 7
What Is Patient and Family Engagement?
Patient and family engagement involves: “collaborating with patients and families of all ages, at all levels of care, and in all health care settings. [Patient and family engagement] acknowledges that families, however they are defined, are essential to patients’ health and well-being.”
Slide 8
How and Where to Engage Patients and Families
- Engaging in planning and design:
- Infrastructure advisory
- Engaging in everyday care:
- How-to strategies
- Engaging with after an adverse event
Slide 9
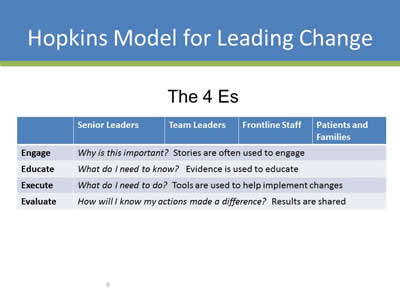
Hopkins Model for Leading Change
The 4 Es
| Senior Leaders | Team Leaders | Frontline Staff | Patients and Families | |
| Engage | Why is this important? Stories are often used to engage. | |||
| Educate | What do I need to know? Evidence is used to educate. | |||
| Execute | What do I need to do? Tools are used to help implement changes. | |||
| Evaluate | How will I know my actions made a difference? Results are shared. | |||
Slide 10
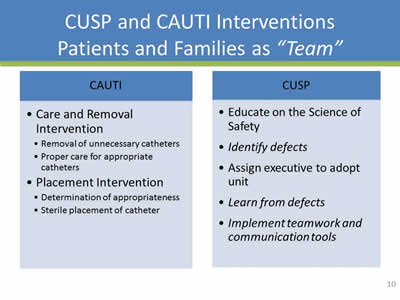
CUSP and CAUTI Interventions Patients and Families as “Team”
CAUTI
- Care and Removal Intervention:
- Removal of unnecessary catheters
- Proper care for appropriate catheters
- Placement Intervention:
- Determination of appropriateness
- Sterile placement of catheter
CUSP
- Educate on the Science of Safety
- Identify defects
- Assign executive to adopt unit
- Learn from defects
- Implement teamwork and communication tools
Slide 11
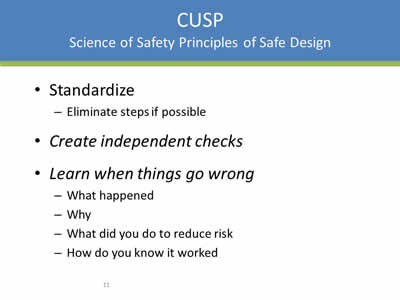
CUSP: Science of Safety Principles of Safe Design
- Standardize:
- Eliminate steps if possible
- Create independent checks
- Learn when things go wrong:
- What happened
- Why
- What did you do to reduce risk
- How do you know it worked
Slide 12
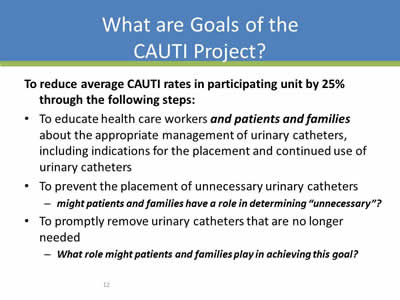
What are Goals of the CAUTI Project?
To reduce average CAUTI rates in participating unit by 25% through the following steps:
- To educate health care workers and patients and families about the appropriate management of urinary catheters, including indications for the placement and continued use of urinary catheters
- To prevent the placement of unnecessary urinary catheters:
- Might patients and families have a role in determining “unnecessary”?
- To promptly remove urinary catheters that are no longer needed:
- What role might patients and families play in achieving this goal?
Slide 13
Principles of Safe Design Apply to Technical and Teamwork
Slide 14
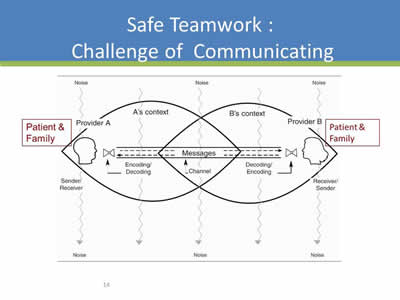
Safe Teamwork: Challenge of Communicating
Image: Graphic showing how communication is coded, decoded, and encoded between the patient and the family and others.
Slide 15
Involving Patients and Family Members as “Team”
- Serve on the CUSP team
- Provide input to improve policies and procedures
- Advise on how to communicate an adverse event to a patient and family members
- Present at staff meetings “stories of care”
Slide 16
Teams Make Wise Decisions When There is Diverse and Independent Input
- Wisdom of Crowds:
- Seek involvement from clinicians at all levels of the organization, and patients and families
- Alternate between convergent and divergent thinking:
- What does everyone think?
- What will be “our” policy/procedure/practice?
- Get from the dance floor to the balcony level:
- Individual challenges
- System challenges
Heifetz R, Leadership Without Easy Answers,1994.
Slide 17
Core Concepts of Patient and Family Engagement
- Dignity and respect
- Information sharing
- Participation
- Collaboration
Slide 18
Dignity and Respect
- Health care practitioners listen to and honor patient and family perspectives and choices.
- Patient and family make-up, knowledge, values, beliefs, religious and cultural backgrounds are incorporated into the care planning and delivery.
Slide 19
Information Sharing
- Health care practitioners share complete and unbiased information with patients and families in ways that are easily understood and address concerns or questions.
- Patients and families receive timely, complete, and accurate information to participate in care and decision making.
Slide 20
Participation
- Patients and families are encouraged to participate in care and decision making at the level they choose.
Slide 21
Collaboration
- Patients, families, health care practitioners, and health care leaders collaborate in policy and program development, implementation, and evaluation
Slide 22
Summary
- Safety is a property of system
- We need lenses to see the system including patient and family lenses
- We need to provide a safe space for all stakeholders, including patients and families to share their voice
- CUSP is a structured approach to learn from mistakes and improve safety culture
- Educating on the Science of Safety is Step 1
Slide 23
Action Items
- Have all members of the CUSP CAUTI Team view the Science of Improving Patient Safety video
- Imagine all of the places where “patient lenses” would add dimension to your improvement efforts
- Develop a plan to invite patients and families to join your team:
- Consult with your CUSP executive to gain support for your plan
- Consider whether the Science of Safety Video might be valuable for patient/family advisors
Slide 24
Additional Resources
CUSP tools are available online by visiting the AHRQ Web site: www.ahrq.gov/cusptoolkit.
Slide 25
The Role of the Patient Experience Advisor
Gail Panoff
Slide 26
Overview of the Council
- Council is a part of Saint Joseph Mercy Hospital Health Systems
- Foundation: around 2010
- The PCEC and St Joseph Mercy Health System share a common goal to assure the voice of the patient and family are heard to help shape how care and service are delivered
- 15 Council members / 55 Patient Advisors
- Our council meets for 2 hours, once a month
Slide 27
Reporting Mechanism (Structure)
- The executive director for patient and community engagement is the champion for this effort and serves on the council
- Council is directly accountable to the executive director of the patient and community engagement at the hospital
- The executive director, chairperson or delegate presents a report to the quality and safety committee of the system board annually on council activities and outcomes
Slide 28
How to Recruit and Become an Advisor
- Recruitment:
- Brochure
- Website
- Hold message
- Referrals
- Service recovery following complaint
- Application process:
- Complete application
- Interview
- Orientation/ training
Slide 29
Roles of an Advisor
- Committee Member- Member on a hospital committee represents the patient or family member perspectives to quality improvement efforts
- Focus Groups- Past patients or family members share perspectives and ideas on specific topics
- Communication Reviewer- Reviews Patient education materials ,newsletters, websites and other materials. Done remotely & electronically
- Experience Sharing- Provides experiences of their health care journey as to learn what is helpful and what is not. Presentations may be at new orientations, educational seminars, dept. or committee meetings, Simulations & Patient Testimonials
Slide 30
Representation of the Patient and Community Engagement Council
- Council Members – 1/3 = staff 2/3 = patients & family members
- Departments include:
- Clinical Quality Safety and Risk
- Nursing
- Service Excellence
- Medical Staff
- Patient and Community Engagement
*Other departments are brought in as needed to learn, observe and participate. Example: representatives from other hospitals and executive leadership participation in meeting*
Slide 31
Representation of the Patient and Community Engagement Council (continued)
- Patients and family:
- Goal: 2/3 patients or family members
- Diversity:
- Very important component
- Age, gender, varied experiences, race, ethnicity, religion- representation from all communities
Slide 32
Contributions of the Council
- Welcome Video to welcome new patients to the hospital
- C- Diff flyer
- Brochure on Pressure Ulcers
- Noise Reduction Sleep Time Sign
- Nurse Residency Program- Testimonials
- Food and Quality Improvements
- Discharge Pharmacy Program
- Patient’s Rights and Responsibilities Brochure
- Patient Discharge Instructions
- Simulations- Disaster recovery (example: tornado)
Slide 33
Councils that Advisors Serve On
- Advisors serve on the following councils:
- NICU CPT
- Stroke CPT
- Pain CPT
- Ann Arbor Quality and Safety Committee
- Ambulatory Patient Experience Committee
- Comprehensive Breast Care Center Steering Committee
- Ann Arbor Patient Satisfaction Improvement Team
- Patient and Community Engagement Council
- Patient Experience CPT
- Rehab Steering Committee
- Cardiovascular Patient Education Committee
- NICU Family Advisory Board
Slide 34
End Result
We believe that by engaging patients and their family members in the care process and improving education about health care needs, patients can continue to take an active role in the decisions that effect their care
Patient and family engagement is a powerful tool for improving all facets of care
Slide 35

Questions?
Image: Large blue button with a question mark in the middle of it.
Slide 36
Funding
Prepared by the Health Research & Educational Trust of the American Hospital Association with contract funding provided by the Agency for Healthcare Research and Quality through the contract, “National Implementation of Comprehensive Unit-based Safety Program (CUSP) to Reduce Catheter-Associated Urinary Tract Infection (CAUTI), project number HHSA290201000025I/HHSA29032001T, Task Order #1.”