

NQS Priority: Effective Treatment
- Most measures of Effective Treatment tracked in the QDR relate to priorities of the Heckler Report. Here, we illustrate effective treatment of conditions that were not priorities of the Heckler Report:
- Chronic kidney diseases.
- Musculoskeletal diseases.
- Respiratory diseases.
Nephrologist Consultation Before Renal Replacement Therapy
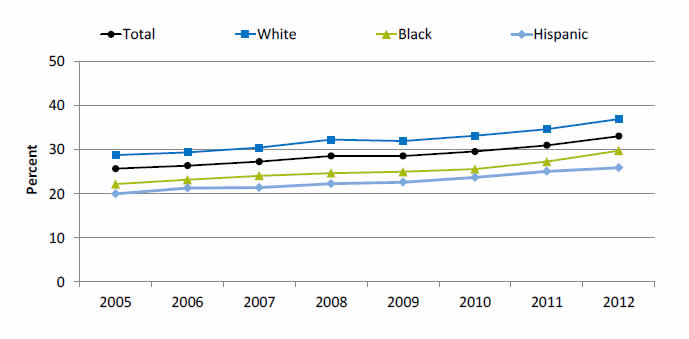
Patients who saw a nephrologist at least 12 months prior to initiation of renal replacement therapy, by race/ethnicity, 2005-2012
| Race/Ethnicity | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 |
|---|---|---|---|---|---|---|---|---|
| Total | 25.7 | 26.4 | 27.3 | 28.6 | 28.6 | 29.6 | 31 | 33.1 |
| Hispanic | 20 | 21.3 | 21.4 | 22.3 | 22.6 | 23.7 | 25.1 | 25.9 |
| Black | 22.2 | 23.2 | 24.1 | 24.7 | 25.0 | 25.6 | 27.3 | 29.8 |
| White | 28.8 | 29.4 | 30.5 | 32.3 | 32.0 | 33.2 | 34.7 | 37 |
Source: U.S. Renal Data System, 2005-2012. http://www.usrds.org/2014/view/v2_02.aspx.
Note: These charts use data from the newest version of the ESRD Medical Evidence CMS 2278 form. The cohorts include incident hemodialysis patients. Includes only patients for whom it is known whether they saw a nephrologist prior to initiation.
- Importance:
- Early referral to a nephrologist is important for patients with progressive chronic kidney disease who are approaching kidney failure.
- Patients who begin nephrology care more than a year before kidney failure are less likely to begin dialysis with a catheter, experience infections related to vascular access, or die during the months after dialysis initiation (USRDS, 2013iv).
- Trends: The percentage of new end stage renal disease (ESRD) patients who began nephrology care at least 12 months prior to initiation of renal replacement therapy improved overall and among Whites but there were no statistically significant improvements among Hispanics and Blacks.
- Groups With Disparities: In all years, the percentage of new ESRD patients who began nephrology care at least 12 months prior to initiation of renal replacement therapy was higher Whites than for Hispanics.
Care for Chronic Joint Symptoms
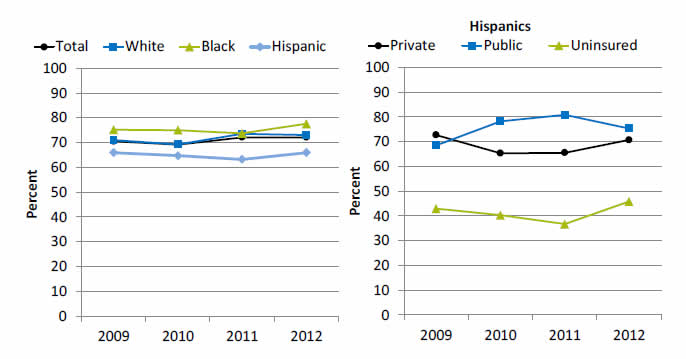
Adults with chronic joint symptoms who have ever seen a doctor or other health professional for joint symptoms, by race/ethnicity and by insurance among Hispanics, 2009-2012
Left Graph:
| Race/Ethnicity | 2009 | 2010 | 2011 | 2012 |
|---|---|---|---|---|
| Total | 70.5 | 69.1 | 72.1 | 72.1 |
| Hispanic | 65.9 | 64.7 | 63.2 | 65.9 |
| Black | 75.2 | 75.0 | 73.7 | 77.6 |
| White | 71.0 | 69.2 | 73.5 | 73.0 |
Right Graph (Hispanics):
| Insurance | 2009 | 2010 | 2011 | 2012 |
|---|---|---|---|---|
| Private | 72.7 | 65.3 | 65.5 | 70.7 |
| Public | 68.5 | 78.2 | 80.8 | 75.3 |
| Uninsured | 42.9 | 40.3 | 36.7 | 45.8 |
Source: Centers for Disease Control and Prevention, National Center for Health Statistics, National Health Interview Survey, 2009-2012.
- Trends:
- In 2012, 72.1% of adults with chronic joint symptoms reported seeing a doctor or other health professional for joint symptoms.
- There were no statistically significant improvements overall or among any ethnic group.
- Groups With Disparities:
- In all years, Hispanics were less likely than Whites to report seeing a doctor or other health professional for joint symptoms.
- In all years, uninsured Hispanics were less likely than privately insured Hispanics to report seeing a doctor or other health professional for joint symptoms.
Completion of Tuberculosis Treatment
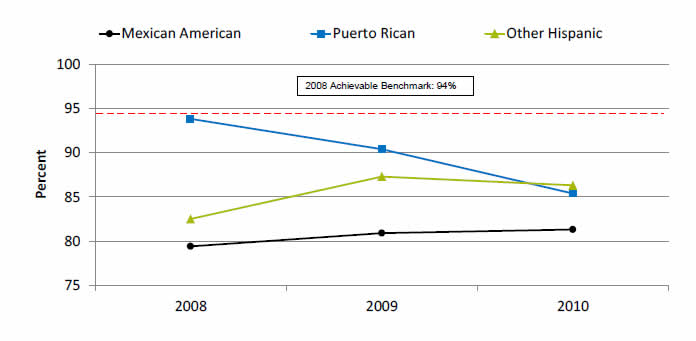
Patients with tuberculosis who completed a curative course of treatment within 1 year of initiation of treatment, by Hispanic group, 2008-2010
| Hispanic Group | 2008 | 2009 | 2010 |
|---|---|---|---|
| Mexican American | 79.4 | 80.9 | 81.3 |
| Puerto Rican | 93.8 | 90.4 | 85.4 |
| Other Hispanic | 82.5 | 87.3 | 86.3 |
2008 Achievable Benchmark: 94%.
Source: Centers for Disease Control and Prevention, National Tuberculosis Surveillance System, 2008-2010.
Denominator: U.S. civilian noninstitutionalized population treated for tuberculosis.
- Groups With Disparities:
- There is considerable variation among Hispanic groups in completion of treatment for tuberculosis.
- Most groups are far from the 2008 top 4 State achievable benchmark of 94%. The States that contributed to the achievable benchmark are Colorado, Kansas, Mississippi, and Oregon.
iv. U.S. Renal Data System. USRDS 2013 annual data report: atlas of chronic kidney disease and end-stage renal disease in the United States. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2013. Available at: http://www.usrds.org/atlas.aspx. Accessed September 19, 2013.
Return to National Quality Strategy Priorities
Return to Contents