

Care Coordination Measures
- Children and adolescents whose health provider usually asks about prescription medications and treatments from other doctors.
- Emergency department (ED) visits with a principal diagnosis related to mental health, alcohol, or substance abuse.
- ED visits for asthma.
Communication About Prescription Medications and Treatments From Other Doctors
- Children are at risk for medication errors, including those due to polypharmacy, for several reasons:
- Their size and physiologic variability.
- Limited communication ability and other factors.26
- Good medical practice includes asking patients about all their medications,27 which can prevent adverse events.
- The Food and Drug Administration and others urge patients to tell health care providers about all their medications.28
- Patients are urged tell health care providers about all their medications.28
- Health care systems are trying strategies to better communicate with patients about medications other health care professionals give them.29
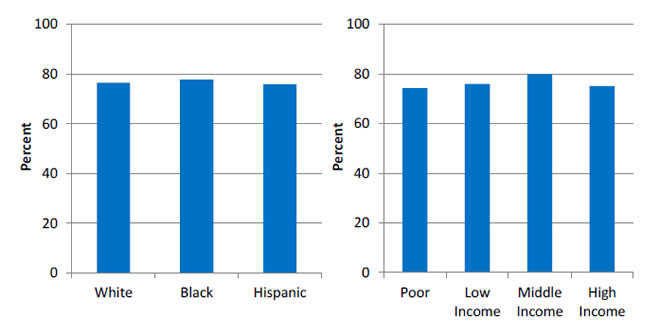
Children and adolescents ages 0-17 years with a usual source of care whose health provider usually asks about prescription medications and treatments from other doctors, by race/ethnicity and income, 2013
Left Chart:
- White - 76.6.
- Black - 77.8.
- Hispanic - 75.9.
Right Chart:
- Poor - 74.3.
- Low Income - 76.1.
- Middle Income - 80.
- High Income - 75.2.
Source: Agency for Healthcare Research and Quality, Medical Expenditure Panel Survey, 2013.
Note: White and Black are non-Hispanic. Hispanic includes all races.
- Trends: From 2002 to 2013, the percentage of children and adolescents whose health provider usually asked about medications and treatments from other doctors increased significantly, from 71.1% to 76.6% (data not shown).
- Groups With Disparities:
- In 2013, there were no statistically significant differences between Whites (76.6%), Blacks (77.8%), and Hispanics (75.9%) in the percentage of children whose health provider asked about medications and treatments from other doctors.
- In 2013, there were no statistically significant differences by income:
- Poor, 74.3%.
- Low income, 76.1%.
- Middle income, 80.0%.
- High income, 75.2%.
Emergency Department Visits Related to Mental Health and Substance Abuse
- EDs are a common source of care for mental illness when high-quality mental health care is not available in the community.30
- Some ED use for mental health and substance abuse problems among young people is seen as preventable with appropriate ambulatory care.
- Mental, emotional, and behavioral health services are lacking for as many as 50% of children and adolescents with high needs.31
- EDs are often not staffed or equipped to provide optimal psychiatric care, leading to long wait times for appropriate care.32
- ED staff observing patients waiting for psychiatric care find it difficult to efficiently care for patients with other medical emergencies.33
- Efforts are underway to prevent avoidable ED use through strategies such as case management.34,35
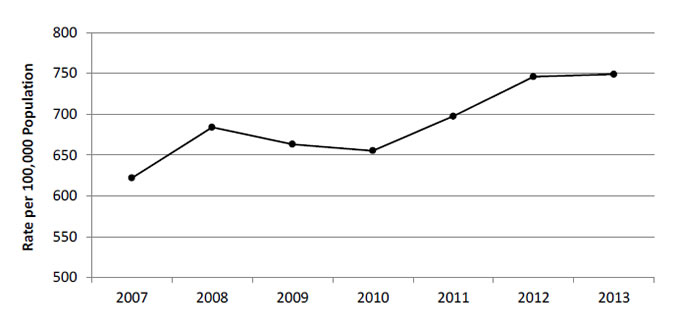
Emergency department visits with a principal diagnosis related to mental health, alcohol, or substance abuse among children ages 0-17 years, per 100,000 population, 2007-2013
| Year | Rate per 100,000 Population |
|---|---|
| 2007 | 621.8 |
| 2008 | 684 |
| 2009 | 663.3 |
| 2010 | 655.3 |
| 2011 | 697.5 |
| 2012 | 746 |
| 2013 | 749 |
Source: Agency for Healthcare Research and Quality (AHRQ), Healthcare Cost and Utilization Project, State Inpatient Databases and AHRQ Quality Indicators, modified version 4.4.
- Overall Rate: In 2013, among children ages 0-17 years, there were 749 ED visits related to mental health, alcohol, or substance use per 100,000 population.
- Trends: ED visit rates for children related to mental health, alcohol, or substance use worsened between 2007 (621.8 per 100,000 population) and 2013 (749 per 100,000 population).
Emergency Department Visits for Asthma
- Asthma is a common chronic disease among children.36
- ED visits for asthma are often preventable if a child receives high-quality ambulatory care.
- Three strategies are most likely to improve provider adherence to guidelines for asthma care:
- Decision support tools.
- Feedback and audit.
- Clinical pharmacy support.37
Emergency department visits for asthma per 100,000 population, children ages 2-17 years, by age, 2008-2013, and by sex and income quartile of ZIP code of residence, 2013
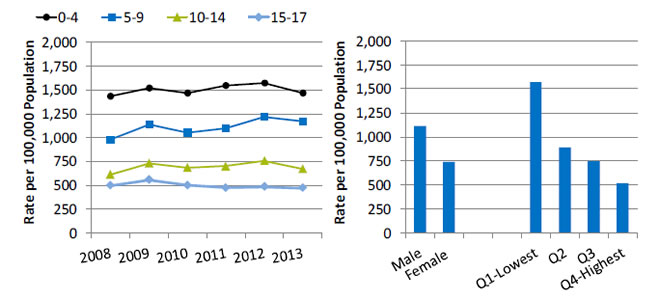
Left Chart:
| Year | 0-4 | 5-9 | 10-14 | 15-17 |
|---|---|---|---|---|
| 2008 | 1432.9 | 978.4 | 609.7 | 496.8 |
| 2009 | 1517 | 1135.6 | 726.2 | 555.9 |
| 2010 | 1465.2 | 1050.1 | 681.4 | 497.7 |
| 2011 | 1545 | 1096.9 | 698.7 | 472.9 |
| 2012 | 1574.3 | 1218.3 | 752.9 | 483.6 |
| 2013 | 1464.4 | 1169.3 | 670 | 471 |
Right Chart:
- Male - 1110.7.
- Female 741.9.
- Q1-Lowest - 1568.7.
- Q2 - 889.8.
- Q3 - 743.8.
- Q4-Highest - 516.4.
Key: Q = quartile.
Source: Agency for Healthcare Research and Quality (AHRQ), Healthcare Cost and Utilization Project, State Inpatient Databases and AHRQ Quality Indicators, modified version 4.4.
- Overall Rate: In 2013, the overall rate of ED visits for asthma was 930 per 100,000 (data not shown).
- Trend: From 2008 to 2013, the rate of ED visits for asthma worsened for children ages 5-9 (from 978 per 100,000 population to 1,169 per 100,000).
- Groups With Disparities:
- In 2013, male children ages 2-17 were 1.5 times as likely as female children to experience an ED visit for asthma (1,111 per 100,000 population vs. 742 per 100,000).
- In 2013, the rate of asthma ED visits was lower for children in the highest income quartile (516 per 100,000 population) compared with children in the first (1,569 per 100,000 population), second (890 per 100,000 population), and third quartiles (744 per 100,000 population).